
Article Figures & Data
Figures
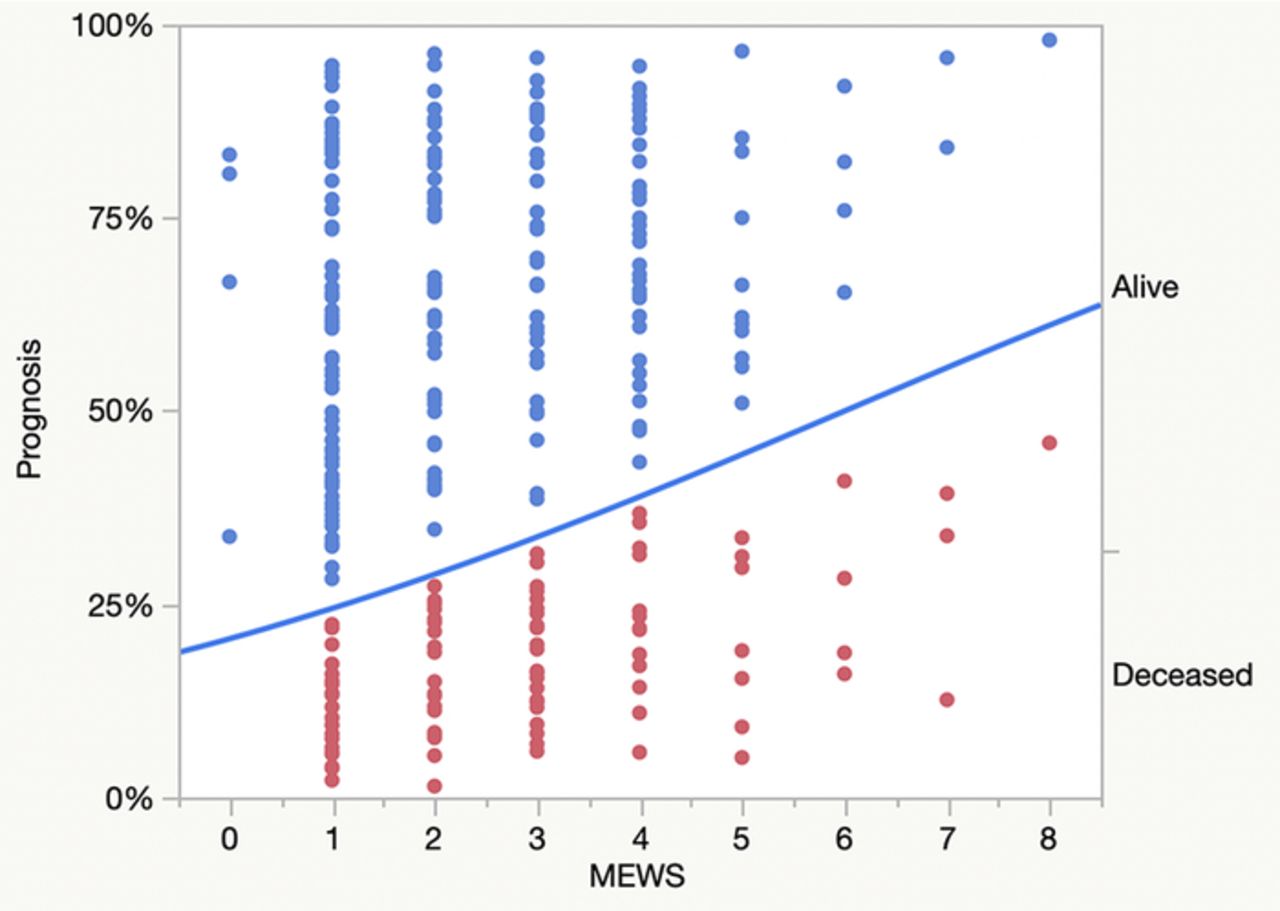
- Figure.
Association of Modified Early Warning Scores (MEWS) on prognosis during unplanned escalation of care. The line plots the probability of prognosis by MEWS values. Points below the line identify deceased patients. Points above the line identify alive patients. The whole-model statistic is χ2=6.5, P=0.0107; C-index=0.60 (confidence interval [CI] 0.54 to 0.66). Following bootstrapping of the model (1,000 cycles), the whole-model statistic was within the CI range (0.56 to 18.3) of probable population values for this clinical setting.
Tables
Bedside Variable All Patients n=263 Age, years, median [IQR] 61 [50-71] Sex, male 144 (55) Body mass index, kg/m2, median [IQR] 26.6 [23.1-33.3] Comorbidities Systemic hypertension 103 (39.2) Coronary artery disease 44 (16.7) History of myocardial infarction 10 (3.8) Nonsinus dysrhythmias 40 (15.2) Coronary artery bypass graft 11 (4.2) Congestive heart failure 46 (17.5) Peripheral vascular disease 56 (21.3) Tobacco abuse 9 (3.4) Chronic obstructive pulmonary disease 20 (7.6) Reactive airway disease 11 (4.2) History of cancer 24 (9.1) Diabetes 65 (24.7) Chronic liver disease 47 (17.9) Chronic renal insufficiency 49 (18.6) Note: Data are shown as counts (%) unless otherwise indicated; IQR, interquartile range, 25%-75%.
Etiology Percentage of Patients n=263 Acute lung injury 33.2 Multiple organ dysfunction syndrome 22.8 Gastrointestinal insufficiency 17.2 Myocardial dysfunction 9.5 Vascular insufficiency 6.5 Acute tubular necrosis 3.0 Airway edema 2.2 Postoperative delirium 2.2 Pancreatitis 1.3 Hemorrhage 0.9 Wound infection 0.9 Splenic injury 0.4 - Table 3.
Probabilities, Associated Calculations, and Cross-Classifications for Testing Across Modified Early Warning Scores (MEWS) in Patients With Unplanned Escalation of Care
MEWS Probability for Mortality, % 1–Specificity, % Sensitivity, % Sensitivity – (1–Specificity), % True Positive, n True Negative, n False Positive, n False Negative, n 8 56.8 0.5 1.3 0.8 1 185 1 76 7 51.5 1.6 5.2 3.6 4 183 3 73 6 46.0 3.8 9.1 5.3 7 179 7 70 5 40.7 8.6 11.7 3.1 9 170 16 68 4 35.6 25.3 29.9 4.6 23 139 47 54 3 30.8 39.3 57.1 17.8* 44 113 73 33 2 26.3 64.5 81.8 17.3 63 66 120 14 1 22.3 97.9 100 2.1 77 4 182 0 0 18.8 100 100 0.0 77 0 186 0 Note: A cut-point of 3 was calculated in this model based upon the highest percentile value in the Sensitivity – (1–Specificity) column.
- Table 4.
Confusion Matrix for Modified Early Warning Score During Bedside Evaluation in Unplanned Escalation of Care
Actual Prognosis Predicted Prognosis Alive Deceased Totals Alive 183 (a or TP) 73 (b or FP) 256 (r1) Deceased 3 (c or FN) 4 (d or TN) 7 (r2) Totals 186 (c1) 77 (c2) 263 (t) ARR, Absolute risk reduction; CI, confidence interval; DP, difference in proportions; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
Prevalence=Alive [c1/t]=186/263=0.707 (71%) (CI 0.65 to 0.76); Deceased [c2/t]=77/263=0.293 (29%) (CI 0.241 to 0.35)
Kappa=0.049 (CI –0.015 to 0.103).
Test statistics not dependent upon prevalence.
Sensitivity=a/c1=183/186=0.984 (CI 0.97 to 0.996)
Specificity=d/c2=4/77=0.052 (CI 0.019 to 0.080)
Positive predictive value=a/r1=183/256=0.715 (CI 0.71 to 0.72)
Negative predictive value=d/r2=4/7=0.571 (CI 0.20 to 0.88)
Positive likelihood ratio=Sensitivity/(1–Specificity)=0.984/(1–0.052)=1.038 (CI 0.99 to 1.08)
Negative likelihood ratio=(1-Sensitivity)/Specificity=(1–0.984)/0.052=0.310 (CI 0.06 to 1.61)
Odds ratio=(a/b)/(c/d)=(183/73)/(3/4)=3.34 (CI 0.61 to 19.4)
Relative risk=(a/r1)/(c/r2)=(183/256)/(3/7)=1.67 (CI 0.89 to 6.08)
Diagnostic odds ratio=[Sensitivity/(1–Sensitivity)]/[(1–Specificity)/Specificity=[0.984/(1–0.984)]/[(1–0.052)/0.052]=3.373 (CI 0.61 to 19.36)
Error odds ratio=[Sensitivity/(1–Sensitivity)]/[Specificity/(1–Specificity)]=(0.984/[1-0.984])/(0.052/[1-0.052])=1,139 (CI 1,711 to 2,553)
Difference in proportions=[(a/r1) – (c/r2)]=[(183/256) – (3/7)]=0.286 (CI –0.09 to 0.60)
Number needed to treat=(1/absolute value of DP) which is equal to (1/absolute value of ARR)=1/0.286=3.49 (CI 1.66 to infinite)
Absolute risk reduction=[(c/r2) – (a/r1)]=[(3/7) – (183/256)]=which is equal to –DP=–0.286 (CI –0.60 to 0.09)
Relative risk reduction=[ARR/(c/r2)]=[–0.286/(3/7)]=–0.668 (CI –5.079 to 0.114)
Youden J value=(Sensitivity+Specificity–1)=(0.984+0.052–1)=0.036 (CI –0.01 to 0.08)
Number needed to diagnose=which is equal to (1/Youden J)=(1/0.036)=27.9 (CI 13.23 to 88.03)
Test statistics dependent upon prevalence.
Accuracy=(a+d)/t)=(183+4)/263=0.711 (71%) (CI 0.69 to 0.73)
Misclassification rate=[(c+b)/t]=(3+73)/263=0.289 (29%) (CI 0.27 to 0.31)
Number needed to misdiagnose=[1/(1–Accuracy)]=[1/(1–0.711)]=3.46 (CI 3.24 to 3.67)









{kind=link}