
Abstract
In August 1999, West Nile virus (WNV), a mosquito-transmitted flavivirus, appeared in New York City. This represented the first time a major outbreak of this Old World virus caused an epidemic in the western hemisphere. By December 2002, the outbreak had spread, probably via avian migratory flyways, to involve 44 states and the District of Columbia. The future epidemiology of WNV infection in the United States will be difficult to forecast. In the absence of an effective human vaccine, the only means of prevention and control is reducing contact between humans and infected mosquitoes. An effective public health infrastructure will be critical in monitoring the progress of this epidemic and developing a strategy to control it.
Louisiana has a long history of being plagued by mosquito-borne infections. As we celebrate the 200th anniversary of the United States making the Louisiana Purchase from France, we are reminded that illnesses like yellow fever and malaria caused significant public health problems in this geographic area long before the real estate negotiations between Thomas Jefferson and Napoleon Bonaparte. In recent years we are seeing regularly what we now term “emerging infections.” These are newly recognized infectious diseases caused by either new infectious agents like severe acute respiratory syndrome (SARS), a corona-virus that may have evolved by genetic mutation from known related viruses, or previously well-recognized infections like West Nile virus (WNV) that for ecologic or biologic reasons have changed the geographic domain that they infect.
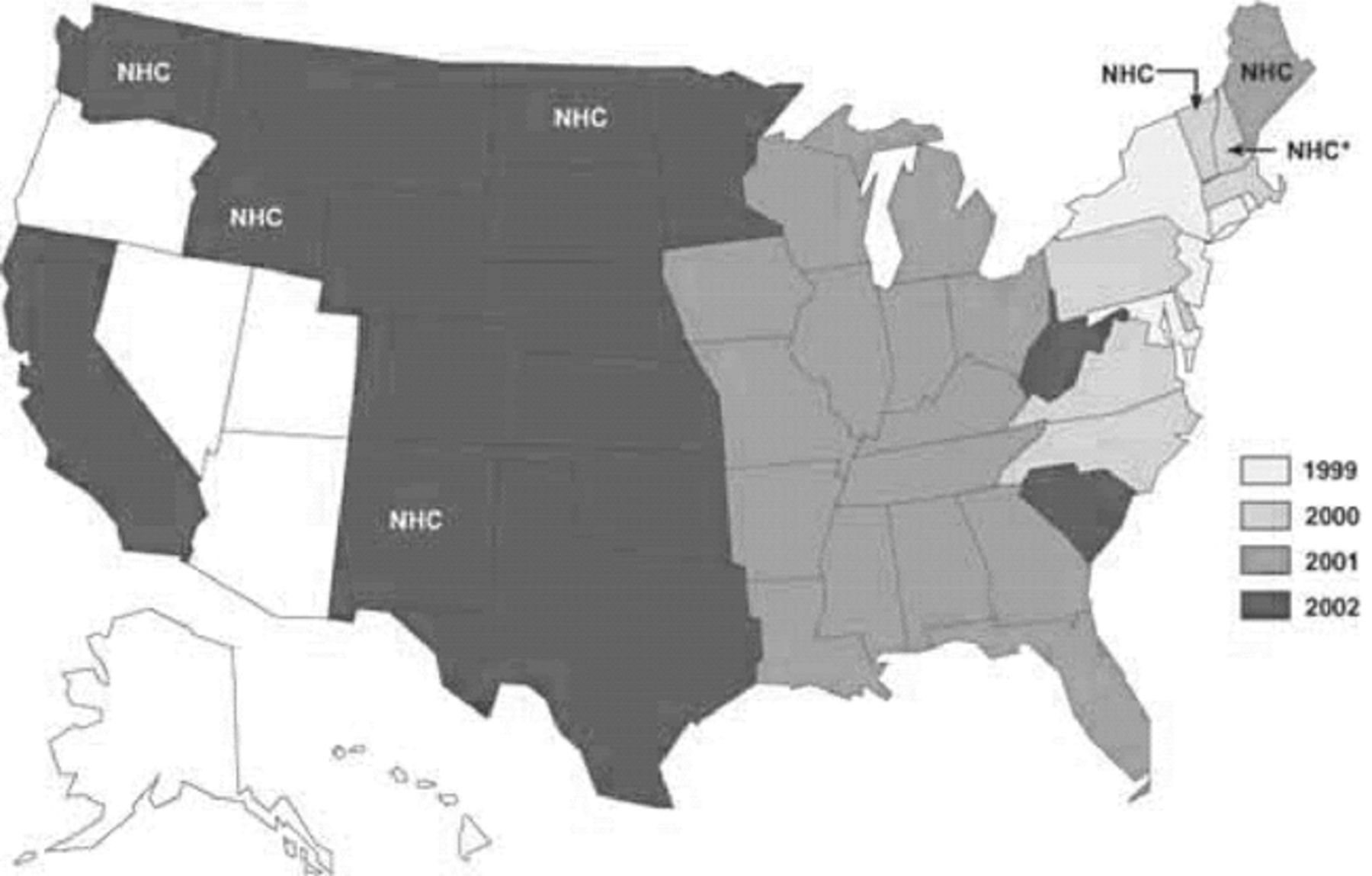
In August 1999, an epidemic of WNV occurred in New York City and two surrounding counties (1). This event marked the first introduction in recent history of an Old World flavivirus into the western hemisphere (2). By 2000, the epizootic had spread to 12 states and the District of Columbia (3), confirming fears that the virus had successfully overwintered and become established in the bird and mosquito population in this part of the United States. By December 2002, the epizootic had expanded in the US to involve 3389 human cases, as well as a large number of infected birds, equines, and mosquitoes in 2289 counties in 44 states and the District of Columbia (Figure). Louisiana had the fourth largest number of reported human cases (319), exceeded only by Illinois (774), Michigan (475) and Ohio (409) (4). Additional epidemiologic and public health concerns were raised when there were reports of transplacental transmission (5), possible transmission by breast milk (6), percutaneous transmission to laboratory workers (7), and transmission through organ donation and blood transfusion (8).

Dr. Dalovisio is President of the Infectious Diseases Society of America.
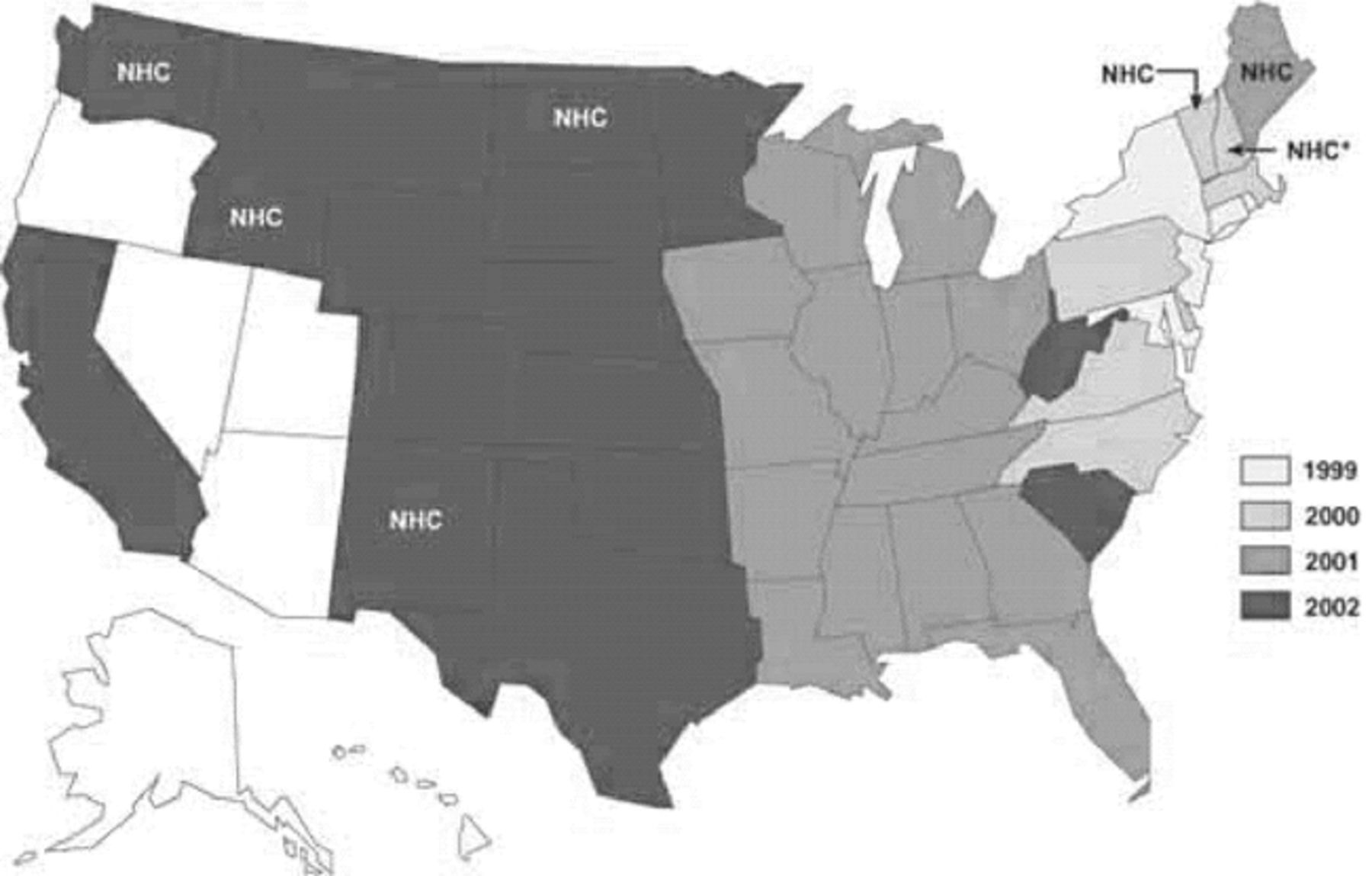
Figure. West Nile virus activity, by state–United States, 1999–2002 (4). NHC = no human cases.
The WNV isolates from the New York outbreak appear to be closely related to WNV isolates from Israel (2). The exact route of introduction of the WNV into the US is not clear. It is clear, however, that the illness has quickly spread across the continental US, probably aided by the broad range of mosquito vectors and avian host species capable of being infected with WNV. Experience with WNV in the Old World may provide clues to the prognosis of the epidemic in the US (9).
However, the future epidemiology of WNV infection in the US will be difficult to forecast. Outbreaks caused by other arboviruses like St. Louis encephalitis, which is closely related to WNV, have been difficult to predict because of the complex ecology of the virus in nature. Factors such as weather patterns, avian migratory patterns, avian mortality from arboviral infection, effectiveness of mosquito control programs, and other unknown variables may alter the behavior of the epizootic.
In the absence of an effective human vaccine, the only means of prevention and control is reducing contact between humans and infected mosquitoes. This includes personal protective measures such as barrier clothing, insect repellants containing DEET (N,N-diethyl-3-methylbenzamide), and avoidance of contact with mosquitoes when possible. Other important strategies are the elimination of conditions favorable for mosquito breeding in inhabited areas such as eliminating standing water collections and urban mosquito control programs. In areas where the epidemic is active, there will be additional challenges to prevent the possibilities (however unlikely) of transmission by transfusion of blood products, organ donation, and maternal-child transmission.
Physicians in areas with enzootic WNV transmission must remain vigilant during the times of the year with WNV activity. Cases may present as undifferentiated fever or viral meningoencephalitis. Awareness of the clinical manifestations of WNV infection and reporting to public health authorities by physicians will be important for tracking future epidemic activity. Health departments need to ensure that lines of communication are open and easy to use between their offices and those of community health care providers. Recent concerns about bioterrorism have heightened awareness of problems with the US public health infrastructure. Hopefully, this increased level of awareness of the problem will result in infusion of resources into the US public health system. Outbreaks of infectious diseases, whether occurring naturally (e.g. SARS, monkeypox, dengue, WNV) or as a result of a bioterrorism event (e.g. anthrax, smallpox) require a robust local, state, and national public health infrastructure to rapidly analyze them and develop appropriate responses.
- Ochsner Clinic and Alton Ochsner Medical Foundation
In this issue








{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.