
Cardiovascular diseases (CVD), including coronary heart disease (CHD), stroke, and heart failure (HF) remain the leading cause of morbidity and mortality in all of western civilization and certainly this is the case in southern Louisiana. In this manuscript, we briefly review some of the preventive cardiology and non-invasive research performed at the Ochsner Heart and Vascular Institute in New Orleans, particularly data from our cardiac rehabilitation and exercise training (CRET) programs, clinical data from our cardiopulmonary laboratory regarding heart failure (HF) prognosis, as well as retrospective data from our cardiovascular informations systems (CVIS), which has allowed us to link a large volume of non-invasive data with subsequent prognosis.
BENEFITS OF CRET
During the past 15 years our institution has contributed significantly to the body of literature available regarding potential benefits of CRET (Table) to improve exercise capacity and overall levels of fitness (which is, in fact, one of the most potent predictors of overall CVD prognosis) in various subgroups of patients (including elderly and women); obesity indices; metabolic syndrome (MS); diabetes mellitus (DM); and plasma lipids (1–24), as well as numerous benefits in the areas of psychological factors (depression, anxiety, and hostility) and overall health-related quality of life (25–33). We have also demonstrated the benefits of this therapy to reduce the risk factor highly-sensitive Creactive protein (HSCRP) (24,34,35), a marker of inflammation, to improve autonomic function (a risk factor for CVD and especially sudden cardiac death or SCD) (36,37), to improve indices of ventricular repolarization dispersion (a marker of increased risk of malignant ventricular dysrhythmias and SCD) (38,39), as well as to reduce levels of homocysteine (associated with increased risk of CHD and stroke) (40) and improve blood rheology (reductions in blood viscosity and improvements in oxygen transport to tissues) (41).
Table - Benefits of Cardiac Rehabilitation and Exercise Training Programs
To further highlight a few of these major findings, we studied 235 consecutive CHD patients following major CHD events who entered and completed CRET and compared them with 42 control CHD patients (following coronary events who did not attend formal CRET) (24). As expected, our CHD patients had moderately elevated levels of HSCRP at baseline (above 3 mg/l), and these levels fell by nearly 40% following CRET (Figure 1). Since statins have been demonstrated to significantly reduce HSCRP, it was important that we also demonstrated that the fall in HSCRP was independent of statin use, occurring equally in the majority of patients treated with statins as well as in those not treated with statins. Since adipocytes or fat cells synthesize cytokines involved in the production of HSCRP, and obesity is known to be associated with high levels of HSCRP which improve with weight loss, it was also important that we demonstrated that the fall in HSCRP following CRET was also independent of weight loss, occurring equally in our patients who lost weight as well as those few who actually gained weight during rehabilitation. We have also demonstrated that our patients with MS have significantly higher levels of HSCRP compared with CHD patients without MS (22,23), and the levels of HSCRP rose proportionately to the number of metabolic factors that are present, reaching very high levels in patients with three – five positive metabolic factors (Figure 2).

Figure 1: Median changes in HSCRP in cardiac rehabilitation and in control CHD patients.24

Relation between number of metabolic risk factors comprising MS and levels of hs-CRP before and after cardiac rehabilitation and exercise training.22
In addition, we believe that behavioral factors and psychological factors have often been under-appreciated as risk factors for CVD and these factors (depression, anxiety, and hostility) are also associated with worse prognosis in patients with CVD (25–33). We have demonstrated a high prevalence of psychological dysfunction in our patients with CHD, with particularly high levels of anxiety and hostility in our younger CHD patients (both older and younger patients have an approximately 20% prevalence of symptoms of depression). All of these adverse psychological factors improve markedly following formal CRET programs, along with the marked improvements that occurred in the rest of the CHD risk profiles in these patients with high levels of psychological distress.
HEART FAILURE (HF) RESEARCH
Our HF / cardiomyopathy group has been extremely prolific in the investigation of patients with HF and cardiac transplantation, and the non-invasive laboratories from OCF have also contributed to these areas of research.
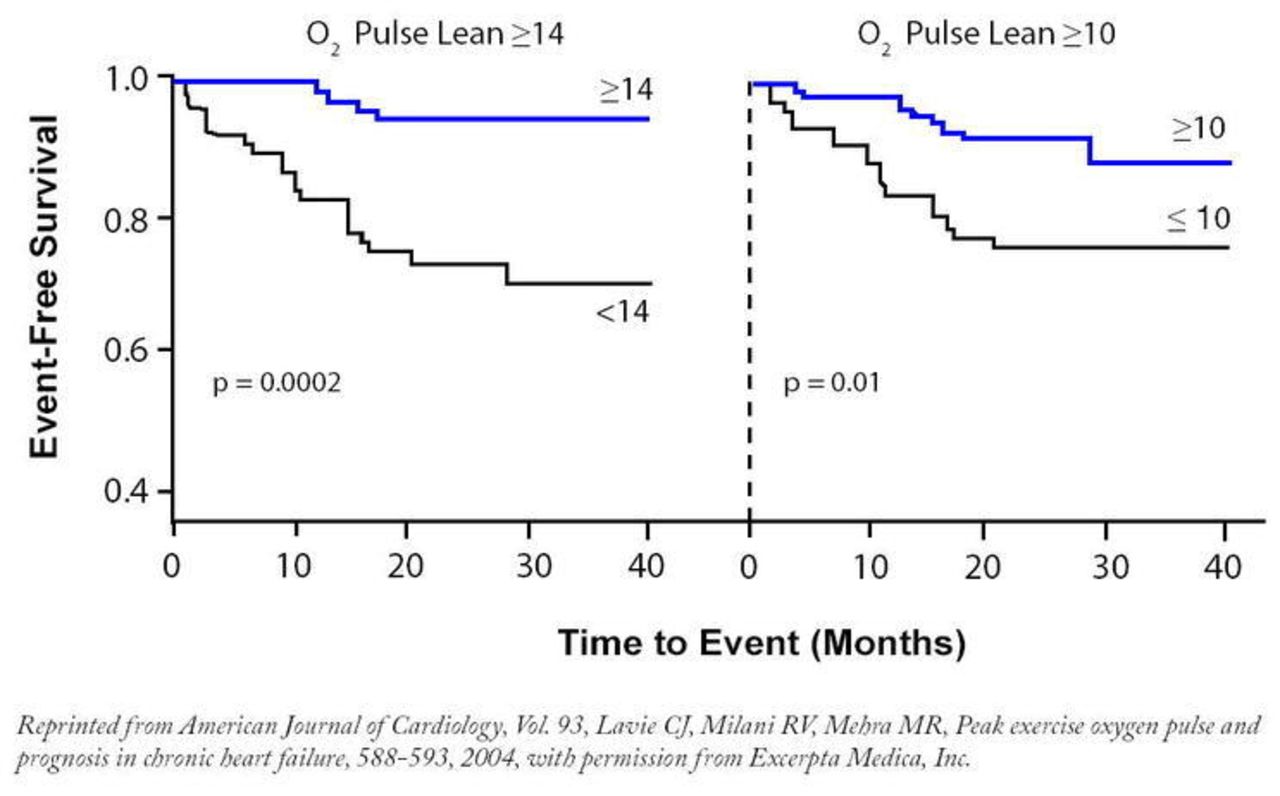
One of the major ways to evaluate patients with severe systolic HF who are being considered for cardiac transplantation is cardiopulmonary exercise testing which provides precise determination of peak oxygen consumption or peak V02 (42–44). Generally, most major HF programs as well as most cardiopulmonary stress testing laboratories correct the peak V02 for total body weight as opposed to lean body mass, although body fat does not utilize substantial aerobic metabolism or perfusion. Several years ago we demonstrated that correcting peak V02 to lean body mass (determined by assessing percent body fat by a number of methods; we use the very simple sum of the skinfold method) performed considerably better than uncorrected peak V02 for predicting cardiac death and need for urgent cardiac transplantation (Figure 3) (45). More recently, we demonstrated that oxygen pulse (peak V02 / peak heart rate, which is a non-invasive marker of stroke volume as well as incorporating the arteriovenous oxygen difference) also performed better than peak V02, more so when correcting for lean body mass (Figure 4) (46).
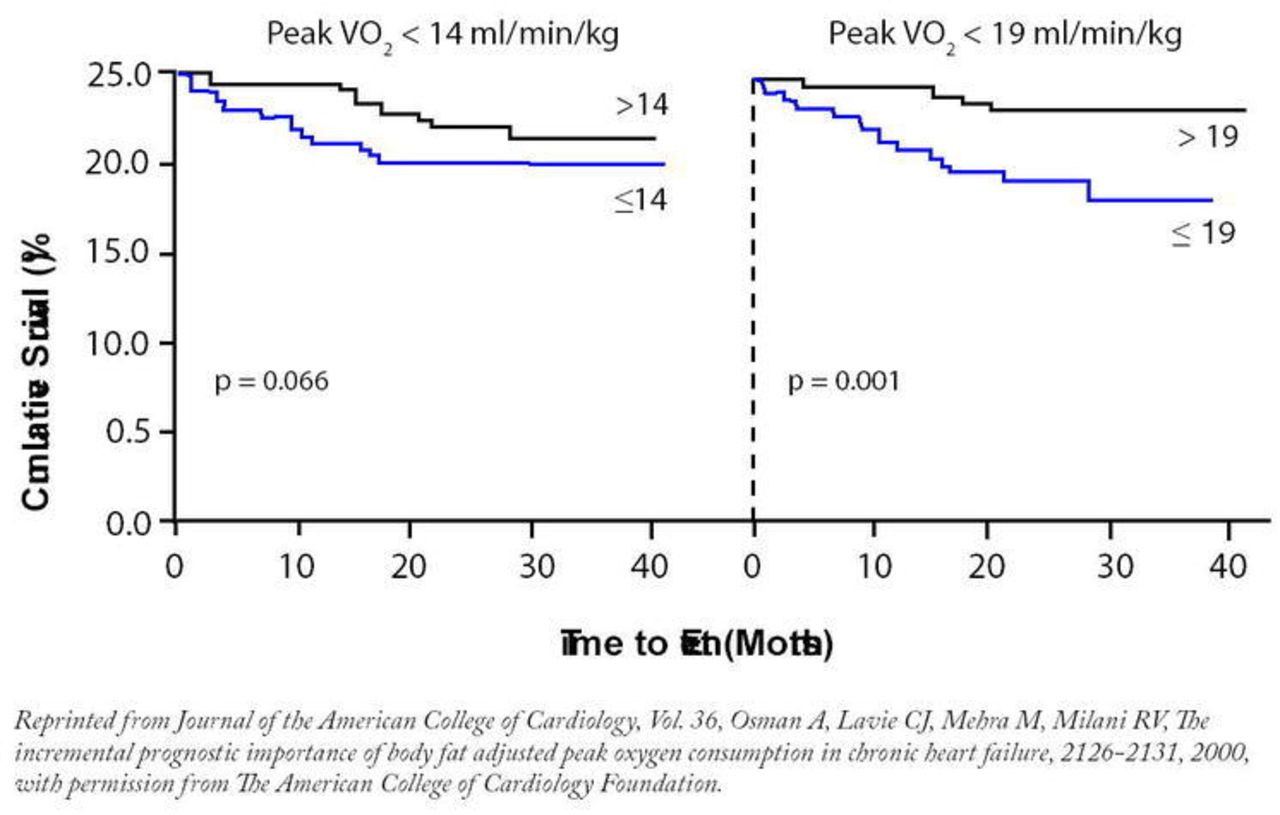
Kaplan-Meier survival curves using both PkVO2 of 14 ml/kg/min and PkVO2 lean of 19 ml/kg/min as cutoffs showing a stronger prognostic value to the fat-adjusted PkVO2 by log-rank testing. PkVO2 = peak oxygen consumption; PkVO2 lean = peak oxygen consumption adjusted to lean body mass; VO2 = oxygen consumption.45

Kaplan-Meier survival curves using both peak O2– pulse 10 ml/beat and peak O2 – pulse lean 14 ml/beat as cut-offs for predicting event-free survival.46
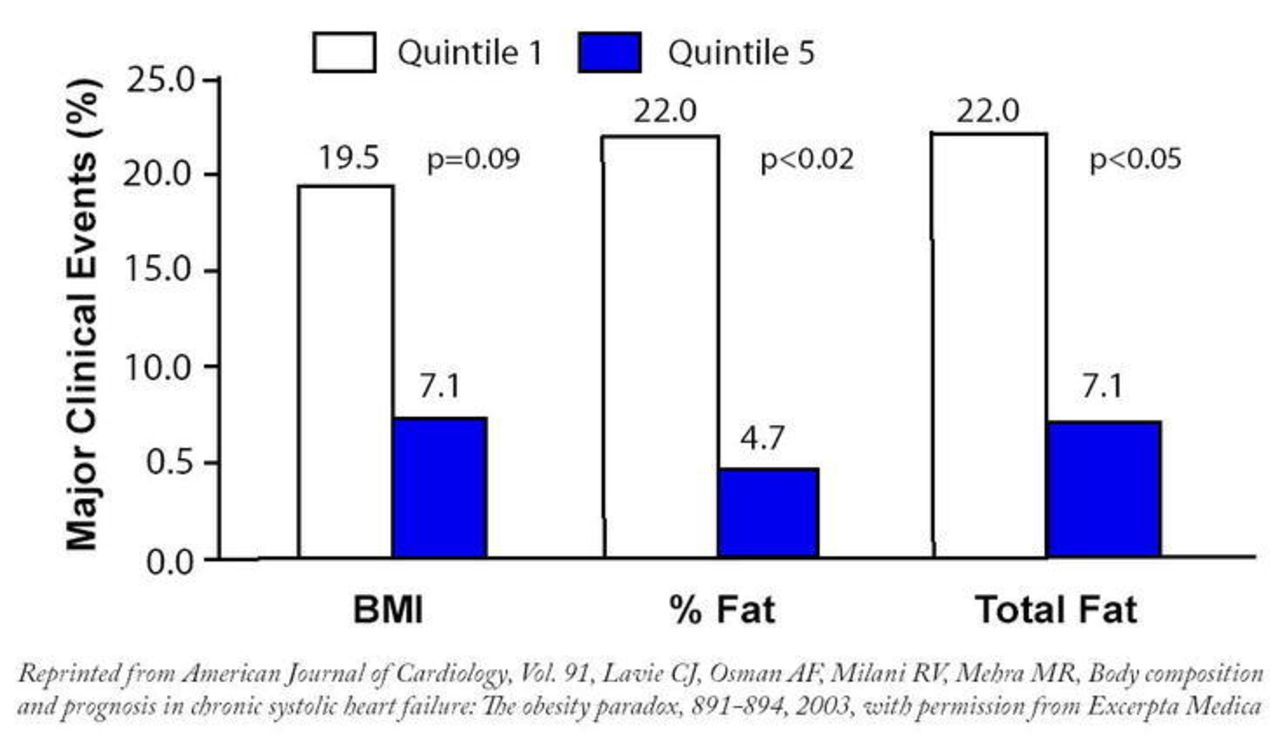
There has also been considerable controversy regarding the role of obesity and pathogenesis of HF as well as HF prognosis (47, 48). Although clearly obesity has adverse effects on cardiac structure and function, and predisposes to the development of HF, we recently demonstrated a paradox regarding obesity and body composition parameters and HF prognosis (47–49). In fact, among our patients with severe systolic HF, those with the highest body mass indices and those with the highest percent body fat had the best prognosis (Figure 5) (49). In multivariate analysis, a higher percent body fat was the strongest independent predictor of event – free survival. In fact, for every 1% increase in percentage body fat, there was a nearly 15% reduction in major CVD events in these patients with severe systolic HF. We believe that these data support the concept of an “obesity paradox” which has also now been demonstrated by others. The reasons for this apparent obesity paradox are uncertain. However, studies have suggested that the natriuretic peptide system and adiposity are closely linked; our group has recently demonstrated reduced natriuretic peptide levels in obese patients with HF (47,50). This lends credence to the explanation that the earlier expression of HF in the presence of obesity could be related to reduced circulating natriuretic peptides. Therefore, obese HF patients may present earlier due to symptoms at a less severe level of HF, therefore promoting discordance between symptoms and prognosis. As we discussed above, it is recognized that peak oxygen consumption with exercise is a potent predictor or prognosis in advance HF and for practical purposes, fat does not consume oxygen or receive substantial perfusion. As we demonstrated above that lean adjusted exercise indices all predict prognosis better than non-fat adjusted variables, this may be particularly applicable to the favorable prognosis in HF patients with a high percentage body fat who generally have relatively high lean-adjusted exercise indices (47,49). In addition, most of the major HF studies, including our own, have not accounted for the effects of purposeful weight loss, which may be associated with more advanced HF and a poor prognosis. Clearly, purposeful weight loss in HF patients with morbid obesity has been associated with improvements in systolic and diastolic function and HF classification, but no large studies have determined the impact that purposeful weight reduction has on HF prognosis and mortality in either patients with preserved or abnormal systolic function (47–49). Finally, other lines of evidence have suggested enhanced protection with obesity against endotoxin/inflammatory cytokines as well as increased nutritional and metabolic reserve (47,50). Certainly, obesity could be associated with a better prognosis in HF and this relationship is not necessarily causal.
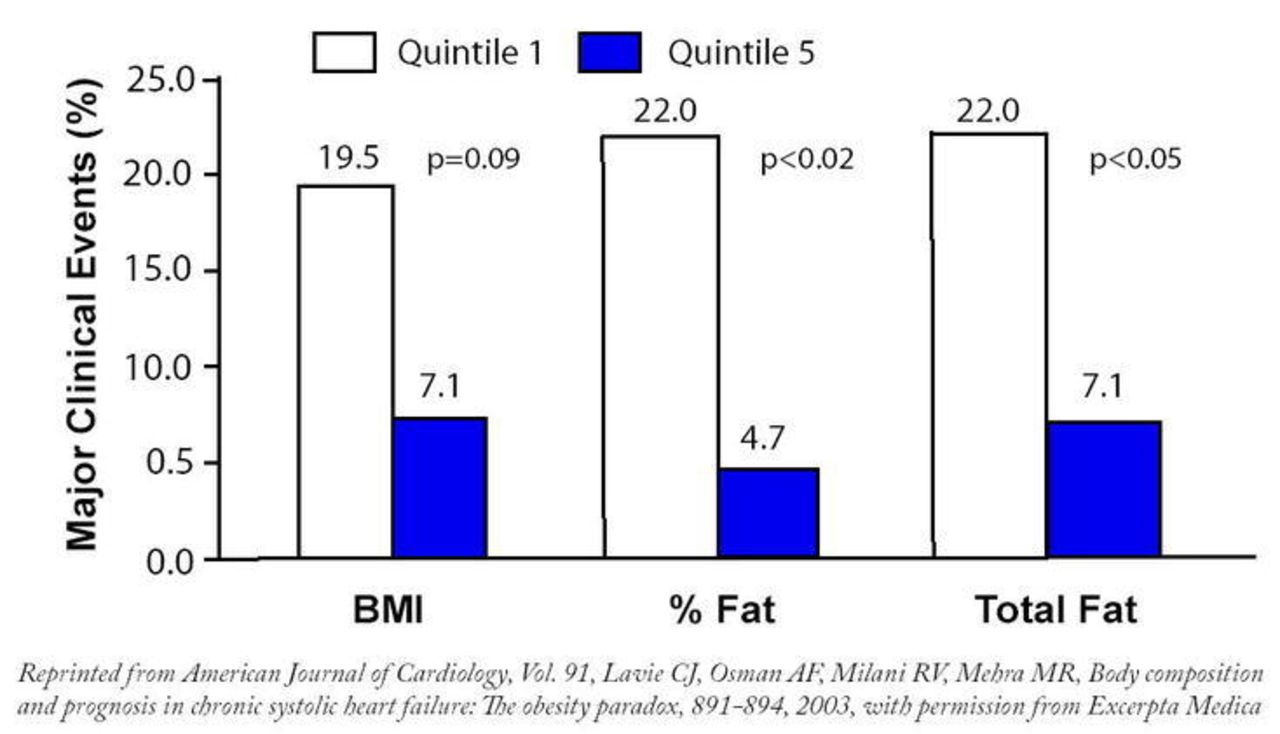
Summary of body composition quintiles comparing major clinical events (cardiovascular death and urgent transplantation) during an average of 19 months of follow-up in the first quintile versus the fifth quintile for BMI, percent body fat (% Fat), and total fat in the total cohort (n=209).49

Carl J. Lavie, MD, Ochsner Heart & Vascular Institute, Department of Cardiology, Ochsner Clinic Foundation
We have also utilized echocardiography to predict allograft rejection in patients following heart transplantation (51) and demonstrated the benefits of statins to reduce allograft rejection and improve survival in these transplant patients (52).
CVIS RESEARCH
Using a robust databank that now includes nearly 75,000 echocardiographic studies of patients who have often been followed for 3–5 years, we have studied the impact of left ventricular geometry (concentric remodeling and eccentric and concentric left ventricular hypertrophy) on survival (53–57) as well as indices of transmural dispersion of repolarization (a marker of increased risk of ventricular dysrhythmias) (58). In addition, we have assessed the prevalence of left ventricular diastolic dysfunction in patients with normal systolic function and the effects on survival (both isolated diastolic dysfunction as well as combined diastolic dysfunction and abnormalities in left ventricular geometry) (59,60). We have also assessed the prevalence of elevated pulmonary artery pressures in patients with structurally normal hearts and the impact of obesity on these increased pulmonary pressures (60,61). We have assessed the impact of valvular regurgitation particularly combined with elevated pulmonary artery systolic pressures on subsequent survival (63), and most recently we have studied a relatively new concept (left ventricular strain and ventricular elastance) in hypertensives and transplant patients, as well as in patients with various left ventricular geometric patterns (64,65). We anticipate that a huge quantity of these data will be published from our non-invasive laboratories in the next several years as this research is ongoing and continuing in the post-Katrina era.
CONCLUSIONS
Although trends indicate that CVD and CHD have been declining during recent decades, these same statistics also tell us that with the aging of our population, the absolute prevalence of CVD is still increasing and the cost of CVD, even adjusted for inflation, is also increasing. Therefore, the prevention and treatment of CVD will continue to be a major emphasis for many years to come. It is hoped that the continued research from these areas at Ochsner Clinic Foundation will at least partly contribute to the prevention and treatment of CVD both locally and at a national level.
- Ochsner Clinic and Alton Ochsner Medical Foundation
REFERENCES
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.