
Abstract
A logical, reasoned approach is essential to the successful management of gastrointestinal hemorrhage. This article describes the approach used by the staff of the Ochsner Clinic Foundation's Department of Colon and Rectal Surgery to evaluate and manage lower gastrointestinal hemorrhage, along with the evidence and experience that guided its development. Following resuscitation, diagnostic studies localize the presence and source of hemorrhage, while management options (non-operative and operative) control the bleeding.
Gastrointestinal hemorrhage can be challenging for any clinician (1). A logical, reasoned approach is essential to successful management. At the Ochsner Clinic Foundation hospital, the majority of patients with gastrointestinal hemorrhage from a lower source have been cared for by the staff of the Colon and Rectal Surgery Department. This article describes the approach used to evaluate and manage these patients along with the evidence and experience that guided its development.
Lower gastrointestinal hemorrhage refers to a spectrum of intestinal bleeding that arises distal to the ligament of Treitz. It may range from occult bleeding or occasional spotting of blood to massive lower intestinal hemorrhage. Massive intestinal hemorrhage typically produces hemodynamic compromise or symptomatic anemia (e.g., hematocrit <30%, transfusion requirements [≥3–5 units of blood/blood products], or orthostasis requiring resuscitation) (2). This bleeding presents challenges, as it can arise from any location in the gastrointestinal tract and may be intermittent and vary in degree (ranging from the passage of 100–250 mL of blood, possibly a few clots and mucous, to copious bleeding with major, self-limited hemorrhage, to massive and continuous hemorrhage associated with hypovolemia) (3). Hemorrhage may present as melena, which suggests bleeding from a source in the proximal colon, small intestine, or stomach; or as hematochezia, which suggests massive left colonic hemorrhage or rectal or anal sources. Massive upper gastrointestinal hemorrhage may present with rectal bleeding due to the blood's cathartic effect and rapid intestinal transit. It is estimated that upper sources present as lower gastrointestinal bleeding in 10% to 15% of cases (2,4). Co-morbidities often complicate the management of gastrointestinal bleeding and must be considered in the diagnostic and therapeutic phases of the care plan.
History and physical examination do not predict patient needs or clinical outcome, and diagnostic studies often are invasive procedures with limited sensitivities and specificities. Patients on anticoagulants or antiplatelet agents for underlying cardiovascular conditions present increased challenges when they experience lower gastrointestinal massive hemorrhage.
Etiologies
Common causes for lower gastrointestinal hemorrhage include colonic diverticula, angiodysplasia, ischemic colitis, and inflammatory bowel disease. Hemorrhage may also come from intestinal tumors or malignancies. Unusual causes of bleeding include nonsteroidal anti-inflammatory drugs (NSAIDS), related non-specific colitis, Meckel's diverticulum, and anorectal diseases.
Initial Assessment, Resuscitation, and Stabilization
Patients with massive lower gastrointestinal hemorrhage may demonstrate pallor, fatigue, angina, tachypnea, cardiac palpitations, postural hypotension, and syncope, which define the significance of hemorrhage and the urgency of clinical attention. Initial resuscitation involves placement of large bore catheters for vascular access, hemodynamic monitoring (cardiac rhythm), and placement of a urinary catheter. Screening for the presence of pre-pyloric, upper gastric sources of bleeding is done through placement of a nasogastric tube, with return of bile on aspiration (5). The goal of resuscitation is to restore volume and replenish red blood cell deficiencies to maintain oxygen delivery. In addition, any coagulopathies must be corrected. Appropriate laboratory studies include a complete blood count, serum electrolytes, a coagulation profile, and a type and crossmatch for blood components.
The diagnostic evaluation begins with a digital anorectal examination and anoscopy. A rigid proctosigmoidoscopy allows the examiner to evacuate the rectum of blood and clots. A complete mucosal assessment serves to exclude internal hemorrhoids, anorectal solitary ulcers, neoplasms, and colitis. Identification of a bleeding source often allows therapy to control the hemorrhage, and this preoperative evaluation aids in intraoperative management if a primary rectal anastomosis is necessary.
After stabilization, the diagnostic evaluation proceeds with three options: radionuclide imaging (nuclear scintigraphy), colonoscopy, and angiography. Colonoscopy and angiography offer therapeutic intervention while nuclear scanning is purely diagnostic. Decisions on the order of testing depend on clinical judgment, local expertise, and the severity or ongoing nature of the hemorrhage.
Patients can be subdivided into three general clinical categories based on the history, physical, and initial laboratory data: 1) minor self-limited, 2) major self-limited, or 3) major ongoing. Major ongoing hemorrhage requires prompt intervention with angiography or surgery. Minor, self-limited hemorrhage may undergo a colonic lavage and colonoscopy within 24 hours. The management of major, self-limited hemorrhage creates the most controversy. Patients with this type of hemorrhage need a diagnostic test to determine if they require prompt therapy or observation.
Radionuclide Imaging
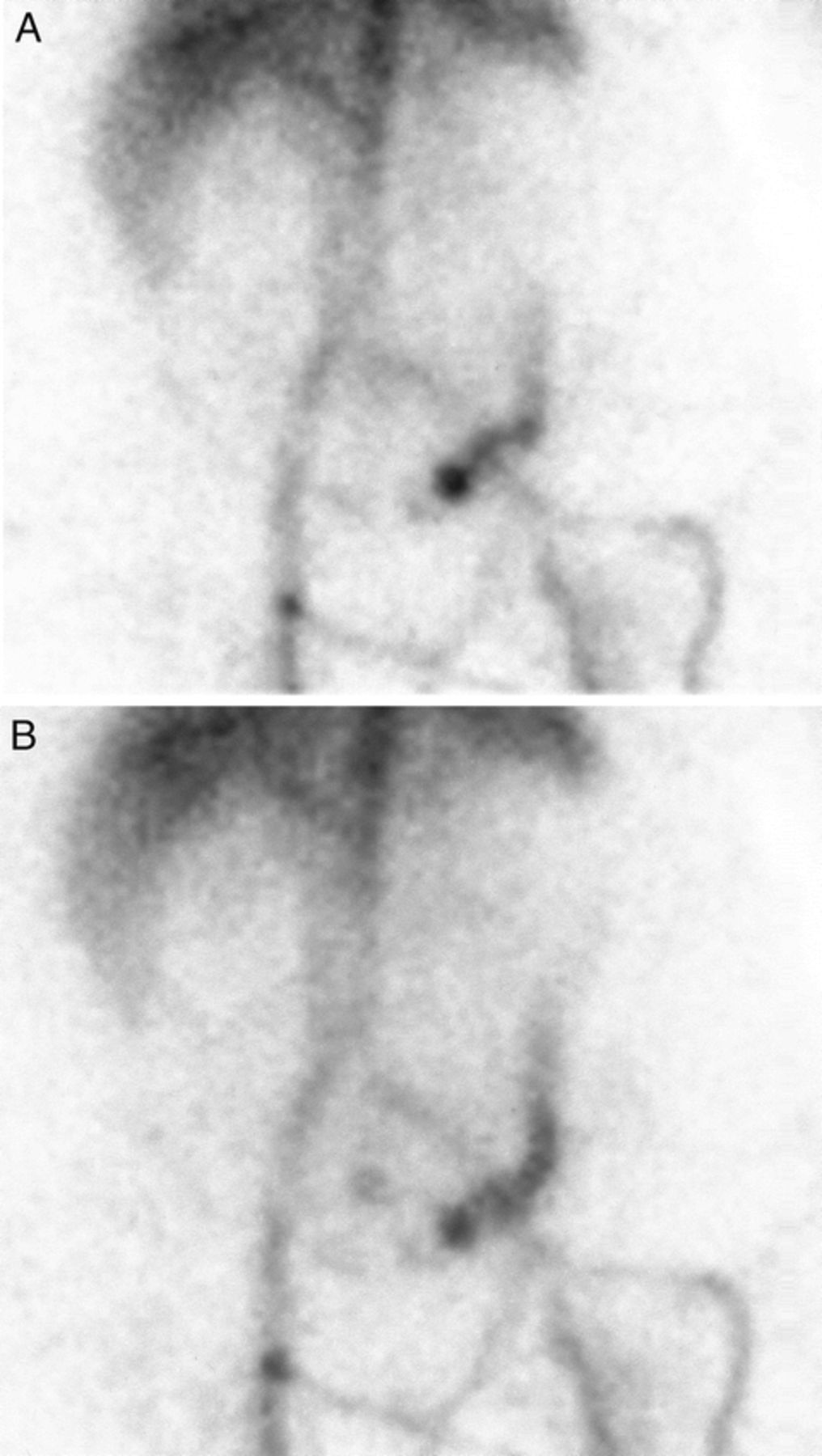
Radionuclide imaging (Fig. 1) detects the slowest bleeding rates (0.1 to 0.5 mL/min). While this technique is more sensitive than angiography, nuclear scanning cannot reliably localize the site of hemorrhage (6). 99mTc pertechnetate-tagged red blood cells (RBCs) is the preferred technique and may cover a period of hours and allow for reimaging within 24 hours. Current reports of nuclear scintigraphy suggest accuracies ranging from 24% to 91% (7). The large variability results from differences in scan timing, technical skills, and experience. Radionuclide imaging is best for patients with major, self-limited hemorrhage (7).

Images from a 99mTc-labeled red blood cell gastrointestinal bleeding study demonstrating extravasation of contrast in sigmoid colon
Experience reported by the Ochsner Clinic Foundation suggests that the timing of the blush predicts the success of angiography (8,9). If the nuclear scan demonstrates an immediately positive blush (within the first 2 minutes of scanning), it is highly predictive of a positive angiogram (60%) and the need for surgery (24%). Just as important, if the initial images do not demonstrate a blush, the study is highly predictive of a negative angiogram (93%) and the need for surgery falls to 7%. Thus, a negative nuclear scan provides objective evidence that the patient is not actively bleeding and may be evaluated by colonoscopy.
Colonoscopy
Many authors believe that colonoscopy has the highest efficacy and should be the first study in patients with major bleeding that appears self-limited (10). Whether colonoscopy should be undertaken emergently depends on the patient's stability. In patients with hypotension and ongoing hemorrhage, it is difficult to safely cleanse the bowel with lavage solutions, and the continued bleeding limits intraluminal visualization and the ability to utilize therapeutic options. In general, these patients require prompt attention with angiography or surgery.
In stable patients with self-limited hemorrhage, colonoscopy is the preferred diagnostic study. The need for bowel preparation is controversial. Colonoscopy without preparation can be described as “emergent,” while administering a mechanical preparation and then performing colonoscopy within 24 hours of presentation is best termed “urgent” colonoscopy. The rapid time preferred for mechanical cleansing usually mandates a lavage method.
Proponents of “emergency colonoscopy” have demonstrated high cecal intubation rates (95%) and a diagnostic accuracy of 72% to 86% (11–13). However, many of the reported series described atypical etiologies for “massive hemorrhage” including ischemic colitis, inflammatory bowel disease, and cancer. The usual rate of bleeding in these conditions is more amenable to urgent colonoscopy (within 24 hours) rather than emergent colonoscopy. Higher bleeding rates are more common with diverticular or angiodysplastic sources.
The benefit of colonoscopy depends on its ability to provide a definitive localization of ongoing active bleeding and the potential for therapy. Many landmarks for colonoscopy may be obscured during hemorrhage. Because of the inability to appreciate all intraluminal landmarks and locate the segment that is bleeding, once the endoscopist highlights a bleeding source, the region of the intestines is best marked with a tattoo of India ink. If the hemorrhage continues and the patient fails medical management, a tattoo greatly assists the surgeon in localizing the hemorrhagic site.
The endoscopist has many therapeutic options to control the bleeding, including thermal agents such as heater probes, bipolar coagulation, and laser therapy. Injection therapy primarily uses topical and intramucosal epinephrine. Mechanical therapy includes endoscopically applied clips (Fig. 2) (2,5).

Clip applied to bleeding diverticular vessel
Angiography
Angiography aids as a diagnostic and therapeutic option in the treatment of intestinal hemorrhage. Acute, major hemorrhage with ongoing bleeding requires emergent angiography, while patients with an early blush during nuclear scintigraphy may benefit from therapeutic angiography. Angiograms may also define a potential source for hemorrhage in occult and recurrent gastrointestinal hemorrhage. In order to appreciate an angiographic blush of contrast, the study requires a hemorrhage rate of at least 1 mL/min (14). Positive yields with angiography range from 40% to 78% (15–18). Appropriate patient selection increases yields and avoids excessive use of angiograms.
The angiographic blush may suggest a specific etiology, but this finding lacks the accuracy of colonoscopy. Highly accurate localization also provides for focused therapy. The hemorrhagic site may receive highly selective, intra-arterial vasopressin infusion. This medication produces potent arterial contraction, which may reduce or halt the hemorrhage. Infusion rates of vasopressin are at concentrations of 0.2 U/min and may progress to 0.4 U/min. The systemic effects and cardiac impact of vasopressin may limit maximizing the dosage. Vasopressin infusion controls bleeding in as many as 91% of patients. Unfortunately, bleeding may recur in up to 50% of patients once the vasopressin is tapered.
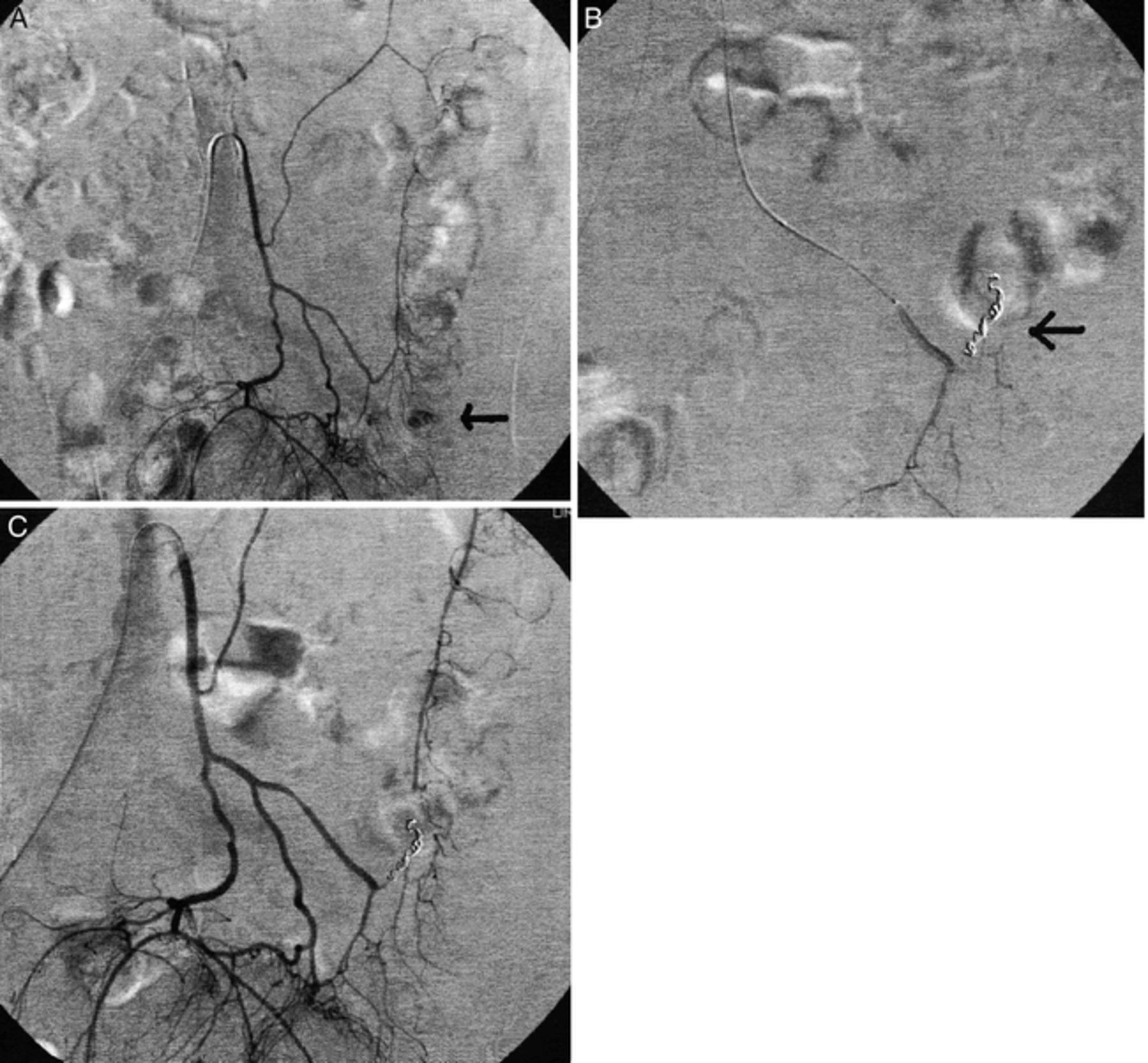
Angiographic technology also allows for arterial embolization to control hemorrhage. Arterial embolization of larger vessels produces intestinal ischemia or infarction in approximately 20% of patients. Much safer super-selective mesenteric angiography using microcatheters allows embolization of the intestinal vasa recta or vessels as small as 1 mm (Fig. 3). Arteriography also has complications, separate from the therapy delivered to the site of bleeding. These include arterial thrombosis, distant arterial emboli, and renal toxicity from the angiographic dye.
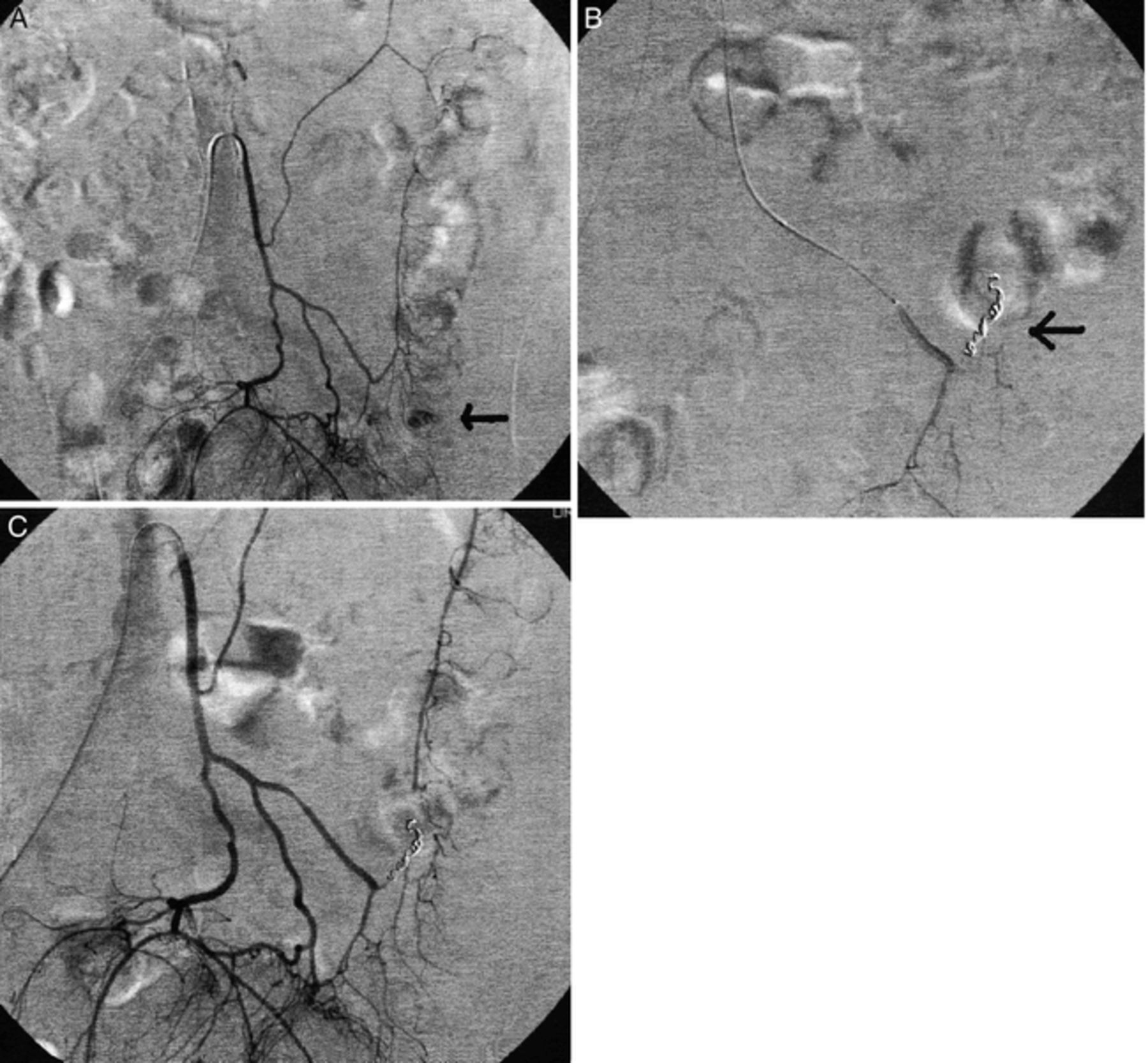
A, Selective angiogram of inferior mesenteric artery demonstrating extravasation (hemorrhage) in sigmoid colon (arrow); B, Angiogram with coil in distal feeding vessel with cessation of bleeding; C, Delayed angiogram demonstrating collateral flow to colon and absence of hemorrhage
Successful embolization therapy provides immediate arrest of the bleeding. Embolization agents include gelfoam pledgets, coils, and polyvinyl alcohol particles (19,20). Success has been better in diverticular bleeds, which are usually fed by one vessel, than with angiodysplasias, which often have multiple feeding vessels.
Newer Diagnostic Methods
Advanced computerized tomography (CT) using thinly sliced, fast image acquisition combined with 3-dimensional software packages has revolutionized the imaging of the vascular tree (21). Vessels smaller than “named” vessels can be visualized, and use of CT angiography has been reported in chronic conditions such as mesenteric ischemia and inflammatory bowel disease (21). Case reports and animal modeling suggest feasibility for gastrointestinal hemorrhage. Image acquisition synchronized with intravascular contrast may outline a site of contrast extravasation or blush defining intestinal hemangiomas, arteriovenous malformations, and angiodysplasias. The sensitivity and specificity of CT angiography in patients with gastrointestinal hemorrhage are unknown and require further research.
Magnetic resonance angiography (MRA) creates images using the bright signal from blood (22). The 3-diminesional images are reconstructed using computerized imaging to project a 2-dimensional image that mimics a conventional angiogram. Further improvement is possible with contract-enhanced MRA (CEMRA). Images using current techniques are not as specific or as refined as an angiogram, but may detect the extravasation of blood pooling in various segments of the intestine. In addition to localizing the site, the study may distinguish small intestine versus large intestine. These studies may prove advantageous when compared to nuclear scintigraphy.
Wireless capsular endoscopy is a diagnostic adjunct for patients with occult hemorrhage (23–26). The first generation capsules are 11 × 30 mm and easily swallowed and tolerated. The current system captures two images per second and transmits the images to a recording apparatus the patient wears. Transmitted images are later reviewed by the endoscopist (Figure 4).

Capsule endoscopy image demonstrating small bowel atriovenous malformation (AVM)
Operative Therapy
Most sources of bleeding spontaneously resolve or are controlled with the current therapeutic interventions. Surgical therapy for intestinal bleeding is rare and associated with significant mortality. Patients who are hemodynamically unresponsive to the initial resuscitation require urgent surgery. In other patients the site of hemorrhage may be localized, yet the available therapeutic interventions fail to control the bleeding. Patient mortality increases with transfusion requirements. Bender et al noted a reduced mortality (7%) for patients requiring less than 10 units of blood, while the mortality increased to 27% for patients receiving in excess of 10 units (27). Therefore, patients with ongoing hemorrhage who require more than 6–7 units of blood during the resuscitation should undergo surgical intervention.
Surgeons should tailor the operative approach based on the preoperative diagnostic evaluations. Surgery starts with a thorough examination of the entire intestine through a large midline, open laparotomy incision. The first objective is location of intraluminal blood with the hope of segmentally isolating a possible source of bleeding.
After the initial visual inspection, the exploration begins in the stomach and duodenum and considers possible missed upper gastrointestinal sources. Next, the small intestine must undergo examination from the ligament of Treitz to the ileocecal valve. Palpation of the intestine may demonstrate such etiologies as a Meckel's diverticulum, ileitis, colitis, or a gastrointestinal stromal tumor (GIST). If the colon appears filled with blood and the small intestine remains spared, the surgeon may focus on colonic sources of bleeding. If the small bowel contains blood, then the operative team has a larger area of concern.
If no source appears obvious after the exploration phase, the surgeon may consider intestinal enteroscopy. The enteroscope or colonoscope exposes the luminal surface and transilluminates the intestinal wall. Transillumination may identify vascular anomalies, small ulcers, or tumors. Endoscopic access to the intestine may require a transoral, transgastric, transcolonic, or transanal approach or a combination of these. Intraoperative endoscopy is a technically difficult endeavor. A team approach with two surgeons or the availability of an experienced endoscopist is important to identify the elusive lesions causing the hemorrhage.
Once the hemorrhage site is identified, an appropriate segmental resection can be performed. If no source of bleeding is confirmed, but appears to arise from the colon, the surgeon should perform a subtotal or total colectomy. Stable patients will tolerate a primary ileosigmoid or ileorectal anastomosis, while unstable patients are best served with an end ileostomy with closure of the rectal stump or a sigmoid mucous fistula.
Critical issues with operative management include delaying surgery until the hemorrhage reaches a critical point beyond 10 units of blood, an associated mortality rate between 10% and 35%, and recurrence bleeding rates of 10% due to imprecise localization of the bleeding (28). Recurrence rates are higher (e.g., 20%) if a limited right or left colectomy is performed without precise localization of the hemorrhage (29). A total colectomy offers the same mortality with a lower chance of recurrent or persistent hemorrhage. Therefore, a total colectomy is the preferred option if preoperative localization is not possible.
Conclusion
The evaluation and management of lower gastrointestinal hemorrhage remains challenging and is best managed with a logical, reasoned approach. An algorithm (Fig. 5) developed by the staff of the Colon and Rectal Surgery Department of Ochsner Clinic Foundation summarizes their evaluation and management of gastrointestinal bleeding.
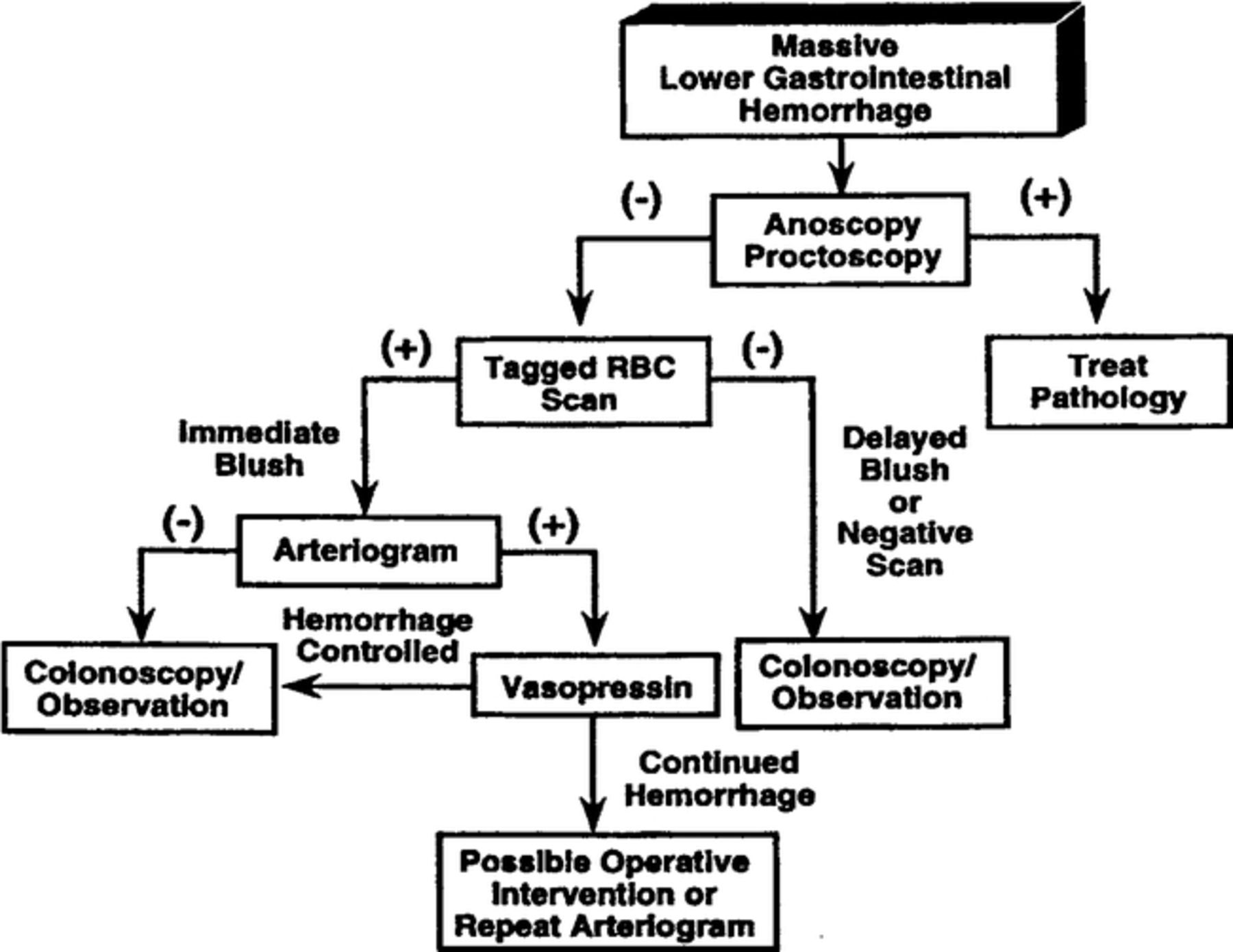
Algorithm for the management of lower gastrointestinal hemorrhage. (From Opelka FG, Gathright JB, Beck DE. Lower gastrointestinal hemorrhage. In Wolff BG, Fleshman JW, Beck DE, Pemberton JH, Wexner SD, eds. ASCRS Textbook of Colorectal Surgery. New York: Springer-Verlag; 2007:299–307. Reprinted with kind permission of Springer Science and Business Media)
Footnotes
Address correspondence to: David E Beck, MD, Chairman, Department of Colon and Rectal Surgery, Ochsner Clinic Foundation, 1514 Jefferson Highway, New Orleans, LA 70121, Tel: (504) 842-4060, Fax: (504) 842-3964, dbeckmd{at}aol.com
- Ochsner Clinic and Alton Ochsner Medical Foundation
References
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.