
Abstract
We review data from epidemiologic and population-based studies that demonstrate the impact of abnormal left ventricular geometric patterns, including both concentric remodeling and left ventricular hypertrophy, on major cardiovascular morbidity and mortality. We also review studies from Ochsner Clinic Foundation that assessed the impact of various left ventricular geometric patterns on overall cardiovascular prognosis, especially all-cause mortality.
For many decades, cardiovascular (CV) investigators at Ochsner Clinic Foundation have focused on left ventricular (LV) hypertrophy (LVH).1,2 Led by the pioneering work of Drs Ed Frohlich and Franz Messerli, considerable work has focused on the causes of LVH, the pathophysiologic consequences of LVH, and the implications for preventing and reducing LVH.1–9 Although initially LVH may be considered as a compensatory effect, since the Laplace law has taught us that increasing LV wall thickness reduces LV wall stress, clearly as LVH progresses, it is associated with considerable CV morbidity and mortality.1–12
Risk Factors
The leading risk factors for LVH are hypertension and obesity, 2 closely related disorders.2–9 Although both obesity and essential hypertension are extremely prevalent and are increasing in our society, each disorder seems to occur more frequently in persons with the other disorder than in a normal population. Obese patients are more likely than lean patients to be hypertensive, and weight gain in a patient with borderline blood pressure will likely lead to the development of definite hypertension. Clearly, the abundance of data now indicates that both of these disorders frequently develop from a common pathophysiologic mechanism (probably insulin resistance), and that obesity begets hypertension and hypertension begets obesity. Other risk factors for LVH are listed in Table 1.3
Risk Factors for Left Ventricular Hypertrophy *
Although both hypertension and obesity strongly affect CV structure and function, early studies from Ochsner demonstrated that the cardiac adaptation to these 2 disorders differed considerably.2–9 The fundamental response to an isolated increase in pressure load or afterload in hypertension is an increase in LV wall thickening without chamber dilatation, whereas obesity, on the other hand, leads to LV chamber dilatation with only minimal increases in LV wall thickness. Since obesity and hypertension are closely linked and often coexist, these 2 disorders often exert a dual burden on the left ventricle, leading to both dilatation and hypertrophy (Figure 1)2 and markedly increasing the premature risk of CV disease.

Consequences Of Lvh
The consequences of LVH are listed in Table 2.3 Our studies from Ochsner have focused on LVH as a risk factor for high-grade ventricular dysrhythmias13–17 as well as for systolic and, particularly, diastolic ventricular dysfunction.15,18,19 Clearly, many epidemiologic and population studies have indicated increases in all CV morbidity and mortality associated with LVH, including coronary heart disease (CHD) events, CHD mortality, and CV mortality, as well as all-cause mortality.4,11,12,20
Consequences of Left Ventricular Hypertrophy *
Detection of LVH
The gold standard for the diagnosis of LVH has involved estimating LV mass (LVM) from echocardiography, where ventricular hypertrophy is defined as a pathologic increase in LV mass.21,22 Landmark studies have determined that echocardiography is extremely accurate for measuring LV wall thickness and chamber dimensions, and these measurements can be utilized to calculate LVM.21,22 Generally, LVM is corrected for body surface area, and LVM index (LVMI) is reported in g/m2.23–25 Some experts, however, have recommended correcting LVM for height or even height2.7 (using 51 g/m2.7 as a cutoff for LVH) to lessen the impact of obesity.26 However, most clinical laboratories and national guidelines for determining LVH have continued to utilize LVMI (g/m2).
LV Geometry
Although the importance of LVH has been recognized now for decades, recent studies have focused on the prognostic impact of more subtle LV geometric abnormalities, particularly concentric remodeling (CR).23–25,27–30 Patients with normal structure have both a normal LVMI (meaning no LVH) as well as normal relative wall thickness (RWT) or low ratio of wall thickness to LV chamber size. Patients with no LVH but an increased RWT meet criteria for CR. Patients who meet criteria for LVH by LVMI criteria have either eccentric LVH (EH) based on normal RWT or concentric LVH (CH) based on increased RWT (Figure 2).27

Recent Ochsner Studies of LV Geometry
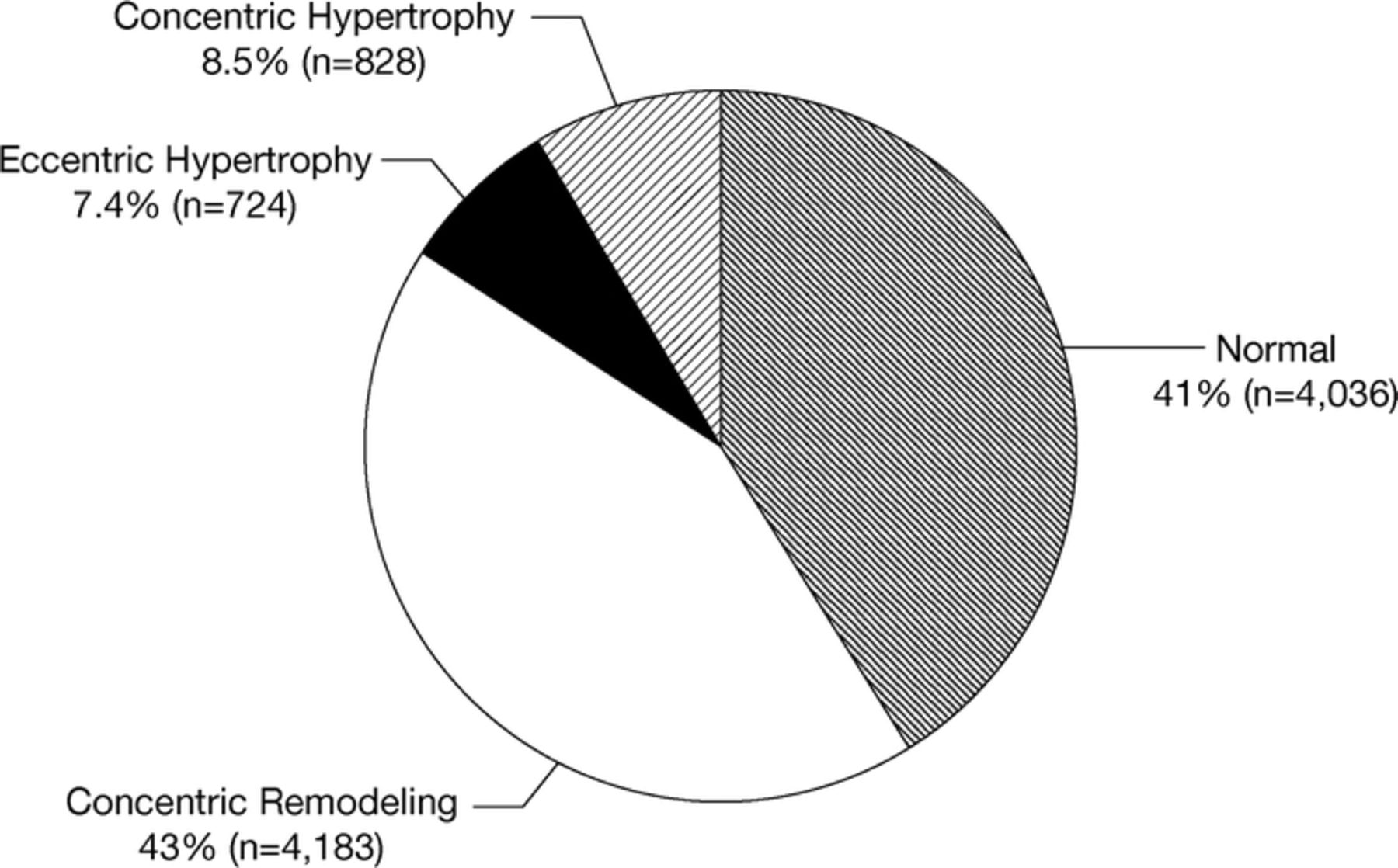
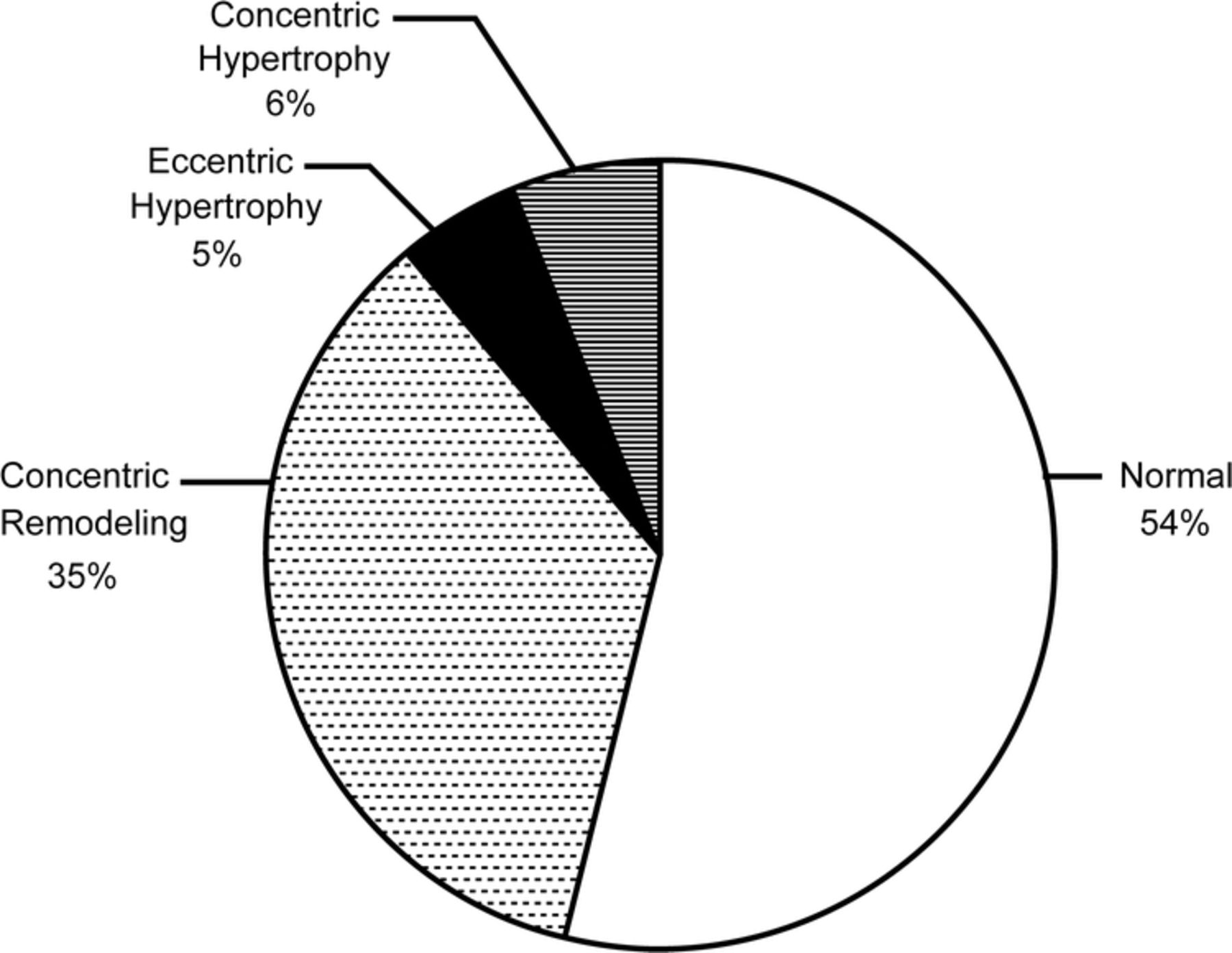
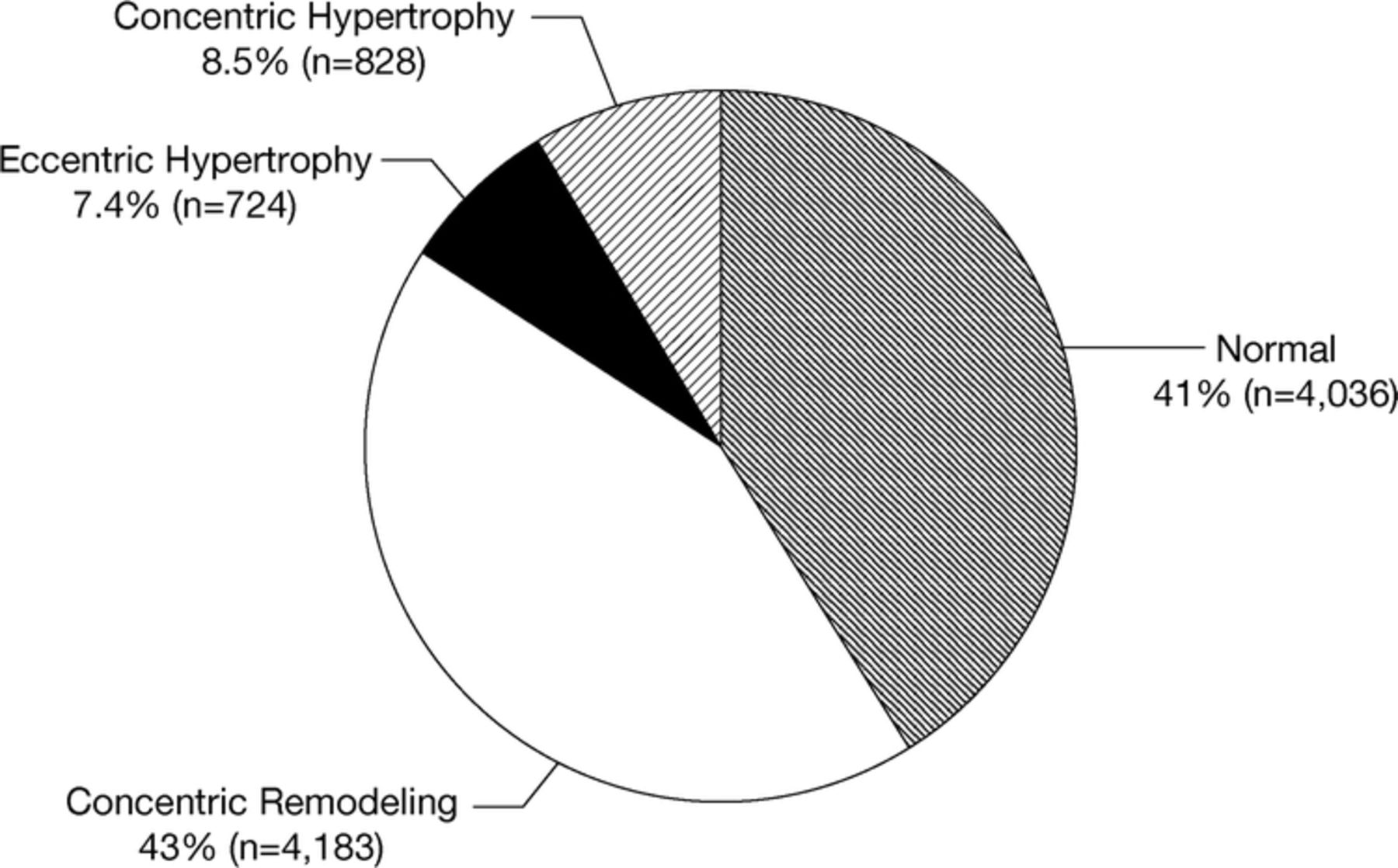
We have recently reported a very high prevalence of LV geometric abnormalities (Figure 3) in patients referred for echocardiography who have preserved systolic function (LV ejection fraction ≥50%),23 with even higher prevalence of LV geometric abnormalities noted in patients 70 years of age or older (Figure 4),24 as well as in obese patients (Table 3).25

Percentage of Left Ventricular Geometric Patterns in Obese and Nonobese Patients With Normal Ejection Fraction Referred for Echocardiography *
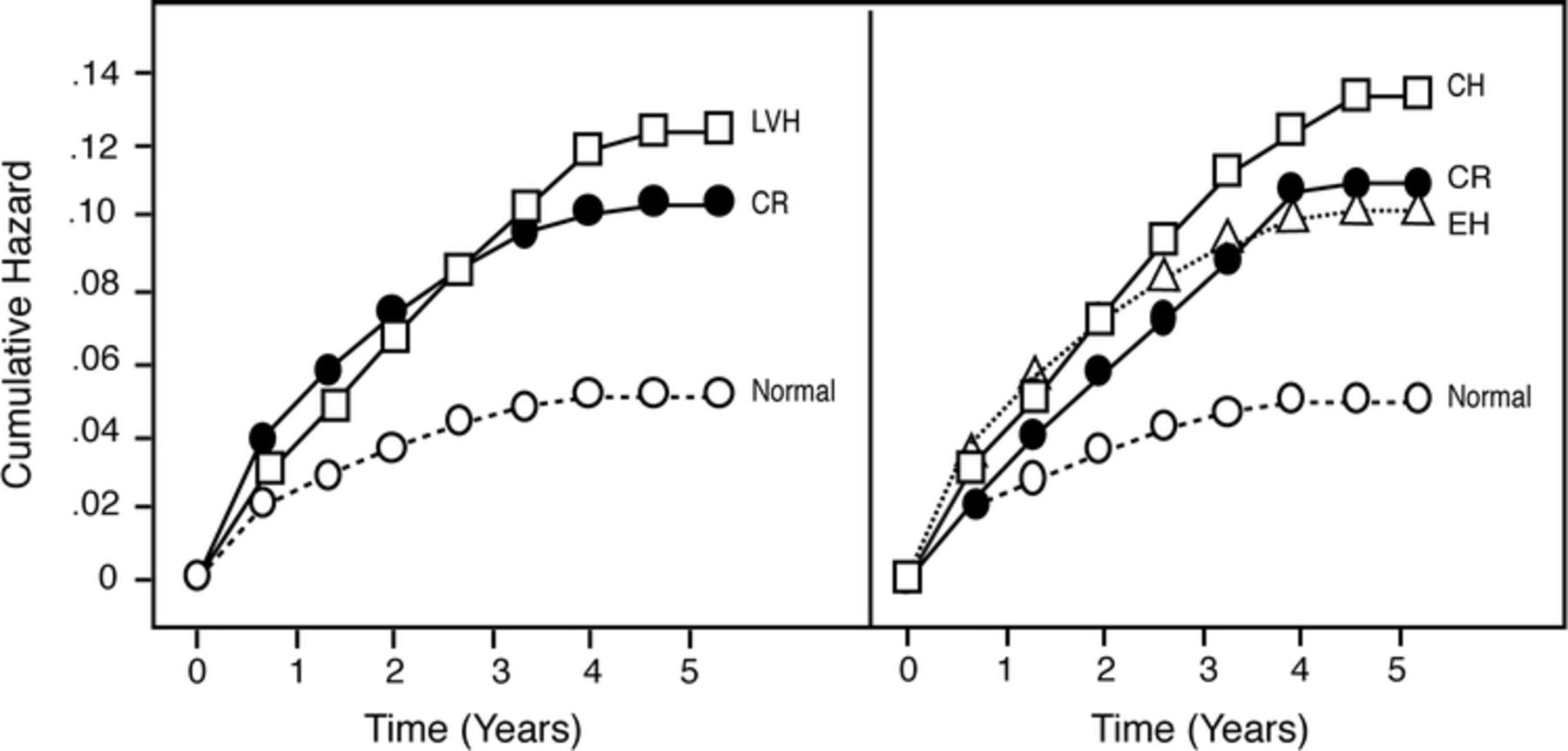
More importantly, our studies have confirmed the adverse prognosis associated with CR as well as with frank LVH.23–25 By assessing all-cause mortality in a very large population, we determined that mortality was increased 2-fold in CR, similar to EH, and was further increased in patients with CH (Figure 5).23 In a study of 9771 elderly patients (age ≥70 y; mean age 78 ± 5 y), mortality was increased by 35% in those with CR compared with those with normal structure and was even 13% higher in CR than in elderly patients with EH, with similar increased mortality in elderly patients with CR and CH (Figure 6).24 Most recently, we reported our findings on obese patients compared with nonobese.25

Although obesity was associated with a higher rate of LV structural abnormalities, as discussed above, the obese had nearly half the mortality compared with nonobese patients.25 This is an example of the obesity paradox that we and others have described during the past decade, which has been noted in patients with heart failure (HF), CHD, and hypertension and now in a cohort referred for echocardiography with preserved systolic function.25,31–36 Nevertheless, in both obese and nonobese cohorts, LV structural abnormalities were associated with increases in all-cause mortality (Figure 7).25 In our entire cohort, higher LVMI and RWT predicted higher mortality, whereas high body mass index (BMI) predicted lower mortality (Table 4).25 However, in the cohort with obesity, a higher BMI predicted higher mortality, suggesting that in marked obesity, higher body weight carries a very poor prognosis, despite the obesity paradox.

Multivariate Predictors of Mortality in Total Cohort (N = 30 920) and in Obese Patients (n = 11 792) with Preserved Ejection Fraction *
Why CR is associated with increased mortality is not totally understood. Concentric remodeling has been associated with an increased arterial load by assessments of arterial compliance and arterial elastance.23–25 Increased RWT, indicating concentric LV geometry, has been associated with high levels of catecholamines, aldosterone, and hepatic growth factors, all of which may increase CV events. In hypertensives with CR, coronary flow reserve may be even more abnormal than in patients with frank LVH. In addition, RWT, more so than LVM, was independently linked to reduced coronary flow reserve. Our studies emphasize this as well by demonstrating that RWT, more so than LVMI, was an independent predictor of mortality in all of the populations studied.23–25 Why CR may predispose patients to an increase in all-cause mortality compared not only with normals but even with EH is not completely understood, but potential mechanisms include elevated arterial load, reduced coronary flow reserve, elevated neuroendocrine components, and abnormal growth factors. Our research suggests that electrical instability and increased ventricular ectopic activity, however, is not the mechanism to explain the increased CV risk associated with CR.37,38
Improvements In Lv Geometry
Some concern has been expressed that if LVH regresses and then hypertensive therapy is discontinued and blood pressure returns to pretreatment levels or even higher, severe HF may occur.1 Indeed, some data from animal studies support this concern, as reviewed by Frohlich from Ochsner.1 However, a study almost 2 decades ago from Ochsner of 19 patients studied before, during, and after LVH reduction demonstrated that despite reintroduction of an increased pressure load, contractile function of the heart remained normal or even improved after LVH reduction.39 Similar studies have documented excellent contractile reserve and diastolic function after reduction of LVH.40–42 Several other studies have documented that reduction of LVH during treatment has favorable effects on overall CV prognosis.41–47
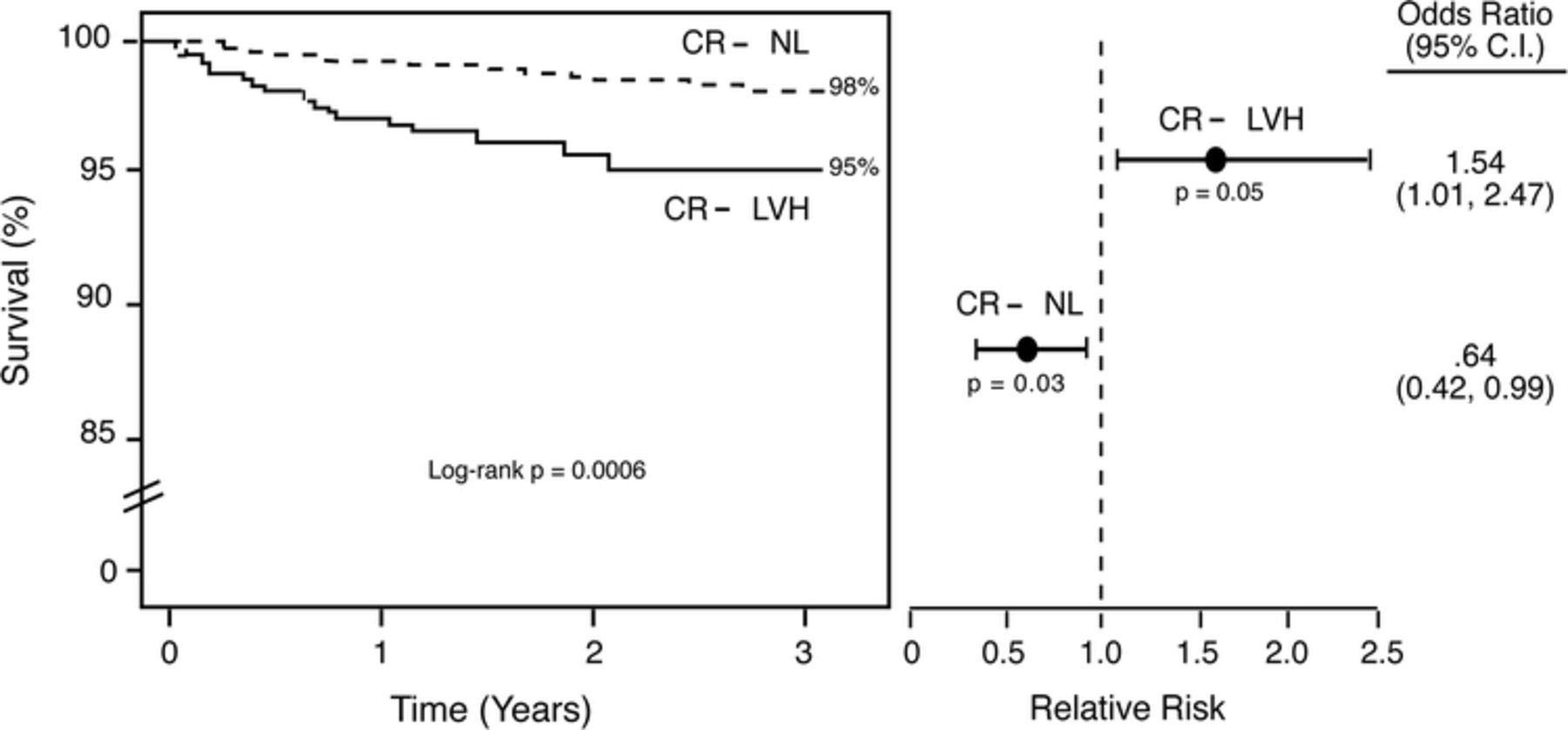
We have recently demonstrated that over time, patients with CR who convert to normal structure have a much better prognosis than those who convert to LVH (Figure 8).23 Therefore, the current data suggest that prevention and reduction of LVH and other abnormal LV geometric patterns, particularly CR, should be associated with an improved overall prognosis.

Lv Geometry, Diastolic Function, and Cv Hemodynamics
Along with LV geometry, we have also assessed the impact of LV diastolic function, including LV relaxation abnormality, pseudonormalization (normal pulse-wave of mitral valve inflow but with blunted or reversed pulmonary venous flow indicating increased left atrial pressure), and restrictive filling, all of which were associated with increases in all-cause mortality.48 Diastolic dysfunction occurs more frequently with abnormal LV geometry, and the combined effects of abnormal LV geometry and LV diastolic dysfunction produced an additive effect on overall mortality.49 Most recently, we also demonstrated that frank LVH (EH and CH) is associated with large increases in stroke work and a large reduction in mechanical efficiency, with similar but smaller changes associated with CR.50
We have also compared cardiac and peripheral arterial stiffening and ventriculovascular uncoupling in 126 normal subjects, 309 with established essential hypertension, and 58 with heart transplantation (HT).51 In essential hypertensives, CR, EH, and CH occurred in 34%, 12%, and 12%, respectively; whereas in HT, CR, EH, and CH occurred in 67%, 5%, and 0%, respectively. Therefore, although HT was associated with a higher prevalence of abnormal LV geometric patterns, these patients had more CR but lower LVH. These HT patients also exhibited evidence of ventriculovascular uncoupling as well as reduced stroke volume indices compared with normal patients and those with essential hypertension.51
Conclusions
Substantial data from Ochsner Clinic Foundation during the past 2 to 3 decades have indicated the prognostic impact of abnormal LV geometry, including both CR and LVH, on overall CV risk. We believe that these abnormal LV geometric patterns, including CR and frank LVH, not only represent a marker of increased CV risk but also serve as a potential target for therapeutic interventions.
- Academic Division of Ochsner Clinic Foundation
References
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- Heart Failure Resulting From Age-Related Cardiac Amyloid Disease Associated With Wild-Type Transthyretin: A Prospective, Observational Cohort Study
- Heart Disease Is Still a Primary Emphasis
- Obesity and Hypertension, Heart Failure, and Coronary Heart Disease--Risk Factor, Paradox, and Recommendations for Weight Loss
- The Russert Impact: A Golden Opportunity to Promote Primary Coronary Prevention