
Most Americans are well aware of the sudden cardiac death (SCD) sustained by television personality Tim Russert recently. Although such tragic events are associated with considerable sadness from many sectors of our society, the medical profession should seize this opportunity as a teachable moment to emphasize and maximize the primary prevention of coronary heart disease (CHD). Within the first few days following his SCD, many clinicians were fielding questions and concerns from patients worried that if this happened to Russert, it might happen to them as well.1
The Event
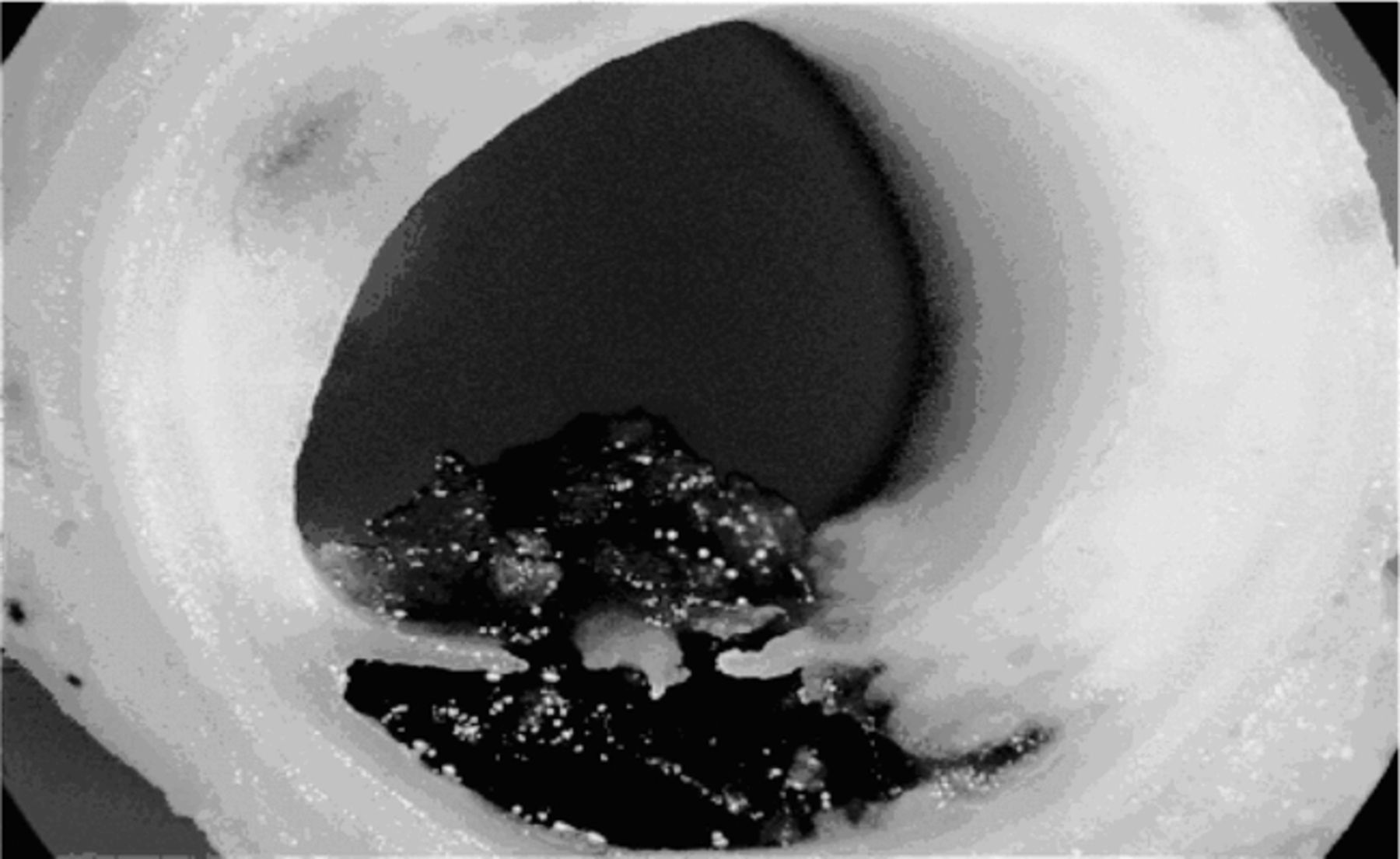
Of the many common risk factors for CHD (Table 1), some were present in Russert (we obviously do not have all of the details of his medical history, although many have been made public knowledge through the media).2 These risk factors may increase the likelihood of developing atherosclerosis over time (Figure 1)3 as well as acute coronary syndrome (ACS) that may manifest as acute myocardial infarction (MI), unstable angina, or, in Russert's case, SCD (Figure 2).4 Years ago, the prevailing paradigm regarding the pathogenesis of ACS hypothesized that it was a progressive buildup of cholesterol within the coronary arterial wall that eventually led to the complete obstruction of the coronary lumen, causing myocardial ischemia and MI. Over the past 10–15 years, however, we have learned that the pathogenesis of most ACS involves inflamed plaque that fissures and/or ruptures, resulting in sudden and rapid thrombus formation (Figure 3). In addition to occluding the coronary lumen, a thrombus can also break off, occluding more distal coronary branches. Although ACS is often considered a sudden event that occurs in seconds or minutes, the pathophysiologic substrate has usually been festering below the surface for weeks, years, and even decades. Surprisingly, in 85% of ACS cases the culprit lesion was less than 70% stenotic prior to rupture and the development of the thrombus, which explains why seeking and eliminating hemodynamically significant stenoses have not proven effective in reducing the risk of MI for patients with stable CHD.5 Finally, although one lesion may cause the ACS, we now know that most of these ACS patients have additional ruptured plaques.6
Risk Factors for Coronary Heart Disease


With ACS, the acutely ischemic myocardium is susceptible to malignant ventricular arrhythmias, including ventricular tachycardia and ventricular fibrillation, thus leading to SCD. Although CHD may present with stable angina pectoris or an abnormal screening examination, unfortunately for many individuals ACS or SCD is the first manifestation. Indeed, for nearly one-fourth to one-half of all CHD patients, SCD is the initial presentation,7 meaning that SCD can be the first, last, and only manifestation of CHD. Although we have no way to know with certainty whether Russert experienced any warning symptoms before his sudden collapse and demise, many such patients do have symptoms that they either ignore or dismiss as unimportant (often mistakenly attributing the symptoms to indigestion or being out of shape).
Risk Factors
To our knowledge, some of which is based on an interview that Russert's primary physician (Dr. Michael Newman) provided to the television program Larry King Live, Russert did not have diabetes and did not abuse tobacco. His hypertension was treated with angiotensin converting enzyme (ACE) inhibitors and later angiotensin receptor blockers (ARBs) in combination with diuretics. Although he had elevated blood sugar levels for years, his most recent fasting glucose was only 104 mg/dL, which placed him in the pre-diabetes category. He was clearly overweight and probably obese (although we do not know his body mass index). Also, he had dyslipidemia characterized by elevated triglycerides (TGs) and low levels of high-density lipoprotein cholesterol (HDL-C), as well as cardiac enlargement (which was discovered during his autopsy but evidently not noted prior to his death). His physician noted that Russert exercised on a cycle ergometer, but we are not certain whether he performed the recommended amount of exercise or had achieved a high level of overall physical fitness. Additionally, we have published many articles regarding the psychological risk factors for CHD, including depression, hostility, anxiety, and overall psychological stress, including work stress.8–19 One might speculate that Russert's very demanding job (involving many tight deadlines, long work hours, inadequate sleep, etc.) engendered a high amount of psychological stress; yet he clearly loved his work and was extremely effective at his job. Nevertheless, psychological factors may have increased his risk for SCD.
Metabolic Syndrome
Metabolic syndrome is an increasingly prevalent condition in our society, estimated to be present in more than 25% of all adult Americans and in approximately 40% of individuals older than 50.20,21 Also referred to as insulin resistance syndrome, metabolic syndrome—which now has its own International Classification of Diseases code (277.7)—is diagnosed when an individual has three or more of the five definition criteria (Table 2).20
Defining Metabolic Syndrome*
The most important criterion for metabolic syndrome is abdominal obesity. Although we are not certain of Russert's exact waist circumference, it was probably in excess of 40 inches and his physician commented that Russert “had increased fat around the belly.” He reportedly had a long history of elevated TGs, although his exact numbers were not reported. He also had low levels (<40 mg/dL) of the protective lipoprotein HDL-C. His physician commented that Russert's HDL-C had improved to 37 mg/dL, but during much of his adult life his HDL-C values were considerably lower, even <30 mg/dL. From a risk factor standpoint, low HDL-C is a stronger predictor of CHD than is either total cholesterol or low-density lipoprotein cholesterol (LDL-C).22 Although his physician indicated that his LDL-C levels had improved (presumably with statin therapy) and his latest value was <70 mg/dL, studies indicate that low HDL-C remains a significant CHD risk factor even with favorable levels of LDL-C.22 Finally, Russert did have pre-diabetes, with a fasting glucose of ≥100 mg/dL, another metabolic syndrome criterion.
By our count, Mr. Russert had at least four and probably all five criteria, and thus clearly met the diagnosis of metabolic syndrome. Patients with metabolic syndrome have a 2- to 12-fold increase in overall CHD and cardiovascular (CV) morbidity and mortality, including SCD, with risk further increased if elevated levels of C-reactive protein (CRP) are present.23 This may not have been known in Russert's case, but CRP levels were likely elevated. Even today SCD is the single most common cause of death, ending the lives of 300 000 Americans each year. Therefore Russert, who in many respects typified the metabolic syndrome patient, was a prime candidate for ACS and SCD.
Cardiac Hypertrophy
The Russert autopsy revealed the presence of cardiac enlargement, though it is unclear whether this was known pre-mortem. We and others have reported that the risk factors for left ventricular hypertrophy (LVH) are hypertension, obesity, and diabetes and that the presence of LVH markedly worsens CV prognosis, even in patients with normal left ventricular systolic function.24–27 Many studies indicate that LVH can be reduced by sodium restriction, weight reduction, and blood pressure control, especially with the use of ACE inhibitors, ARBs, and calcium channel blockers.24
Other Tests
A growing body of evidence indicates that an elevated level of CRP is associated with an increased risk of atherosclerosis and, particularly, an increased risk of acute CHD events.28 Many patients with abdominal obesity and metabolic syndrome have increased CRP levels, further increasing their risk.23,28 A soon-to-be-published trial—the Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER)29 study—demonstrated a substantial benefit of statin therapy in men without CHD who had relatively low LDL-C of <130 mg/dL (average: 108 mg/dL) but elevated CRP of >2 mg/dL. Other therapies, beyond statins, that lower CRP and improve CV health and prognosis include exercise and weight loss.
Another potential test for assessing CHD risk is treadmill stress testing. In an analysis of men from the Cooper Clinic in Dallas, we recently reported that a positive exercise electrocardiogram (ECG) test predicted CHD and CV mortality in 2854 men with diabetes30 and in 9191 men with metabolic syndrome.31 However, we are told that Russert passed an exercise stress test just 2 months prior to his death. Based on his autopsy results this is not surprising, because he did not have significant coronary stenosis other than the one lesion that acutely thrombosed at the time of his SCD. Likely, this lesion was <50% stenosed 2 months earlier and therefore did not produce a positive exercise ECG response (and likely would not have produced abnormal results on a stress imaging study such as an exercise ECG or exercise nuclear perfusion imaging).
Finally, Russert could have obtained a coronary calcium scan. He reportedly had one 10 years ago that showed a calcium score of more than 200, which indicated that Russert had a moderate amount of calcified coronary plaque even then. Based on this, physicians would have recommended that he improve his risk factor profile and obtain an exercise stress test (which he did have and had passed). Coronary calcium scanning is generally extremely effective in evaluating early atherosclerosis and CHD risk. Also, testing is now much more affordable, costing more than $1000 many years ago and only $250 at our institution now, and can affect disease management for many patients. However, in all likelihood this would not have substantially changed Russert's overall clinical management.
Treatment
The prevention of atherosclerosis and major CHD events involves a multifaceted approach.2 Certainly, most high-risk patients should be treated with antiplatelet therapy, such as low-dose aspirin of 81 mg/d,32 unless there are significant contraindications, such as major bleeding or severe peptic ulcer disease. News reports have indicated that Russert was taking low dose aspirin. More vigorous antiplatelet therapy with clopidogrel of 75 mg/d is probably more effective than aspirin,33 but based on cost-effectiveness he would not have met the criteria for receiving this medication, since he did not have a history of major CV clinical events. In addition, in primary prevention the combination of aspirin and clopidogrel is more dangerous than aspirin alone,34 although this combination therapy has not been specifically studied in patients with stable atherosclerosis.
Clearly, nonpharmacological therapies to raise HDL-C and lower TGs would have been appropriate, including regular exercise training (at least 30 minutes on most days) and weight reduction (dietary restriction of calories as well as regular exercise).21,22,35 Even in the obese increased fitness levels have predicted a more favorable CHD and CV prognosis.36,37 Also, unless Russert had a potential for abuse, low doses of alcohol (eg, 1–2 alcoholic drinks/day) effectively increase HDL-C and improve insulin sensitivity and metabolic syndrome, thus reducing the risk for CHD and CV events.38
Regarding metabolic syndrome, we have demonstrated that in our CHD patients cardiac rehabilitation and exercise training have resulted in a significant reduction in metabolic risk factors and a 37% reduction in the prevalence of metabolic syndrome.21 In addition, this therapy dramatically reduces CRP levels in patients with and without metabolic syndrome.21,28 Likely in Russert's case pharmacological therapy to improve dyslipidemia in metabolic syndrome—including niacin therapy or fibrates (gemfibrozil or fenofibrate) that increase HDL-C and reduce TGs—would have been effective.39 However, clinical trials of such therapies have not been performed in patients with ideal levels of LDL-C.
Substantial evidence demonstrates that ACE inhibitors, particularly ramipril, provide substantial CV protection.40,41 This evidence is especially powerful in patients who are post-MI as well as in those with heart failure (HF) or with diabetes. However, in at least one trial, ramipril provided protection against major CHD and CV events, including stroke, in patients with stable atherosclerosis who did not have prior MI, diabetes, HF, or even hypertension (which Russert had).40 Moreover, substantial evidence shows that ACE inhibitors and ARBs reduce the subsequent risk of developing diabetes by approximately 25–30%,42 which may be especially helpful in patients with metabolic syndrome.
Finally, we have recently published several articles supporting the potential cardioprotective effects provided by omega-3 fatty acids or fish oils.43–45 Fish oils produce many beneficial CV effects, but the predominant benefit appears to be related to the prevention of high-grade arrhythmias. This therapy improves autonomic function, augments vagal tone,46,47 and reduces the risk of arrhythmias associated with coronary occlusion/reperfusion. For example, in animal studies, occlusion of the left anterior descending artery produces ventricular fibrillation nearly half of the time. If the animal is pretreated with fish oils, there may be a 60–80% reduction in malignant arrhythmias. The animal may still sustain an MI, but the risk of fatality may be substantially reduced. This effect may be particularly applicable to the Russert case and in other patients with ACS and SCD. Fish oil therapy may reduce the risk of MI in the first place, but more importantly it reduces the risk of malignant arrhythmias and SCD.
Conclusion
Although Tim Russert's ACS and SCD represent a sad and tragic event, the publicity generated by this high-profile death offers clinicians an opportunity to promote the importance of primary prevention of CHD, including assessing risk factors, identifying patients with a high risk of CHD, and providing a multifaceted approach to CHD prevention.
- Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}
{kind=link}