
Abstract
In most cases, a left bundle-branch block pattern on an electrocardiogram is a postoperative phenomenon. Under rare circumstances, it can be found in patients after myocardial infarction or in patients with hypertrophic cardiomyopathy, or it can be exercised induced. We describe a pediatric patient with propionic aciduria, dilated cardiomyopathy, and rate-dependent left bundle-branch block on her electrocardiogram.
- Bundle-branch block
- cardiac manifestations in propionic aciduria
- exercise-induced (rate dependent) bundle-branch block
- heart block
- normal heart conduction
- propionic aciduria
CASE REPORT
A 15-year-old girl had a history of propionic aciduria and dilated cardiomyopathy. Her medical history was significant for a severe acidosis episode as an infant that required extracorporeal membrane oxygenation support. During that hospitalization, she was diagnosed as having propionic aciduria. Her family history was negative for sudden cardiac death, arrhythmias, or bundle-branch block.
On physical examination, she was acyanotic and slightly small at the 25th percentile for weight and at the 9th percentile for height. Her lungs were clear bilaterally. Her cardiac examination revealed quiet precordium with a normal first heart sound; her second heart sound was split with a normal pulmonary component. There was a grade I/VI systolic ejection murmur at the left lower sternal border. There was no hepatosplenomegaly, and her peripheral pulses were normal with no brachiofemoral pulse delay.
An electrocardiogram showed sinus rhythm with a left bundle-branch block at a heart rate of 100 beats/min with a QRS duration of 144 milliseconds (Figure 1). Her echocardiogram demonstrated a mild dilated left ventricle (end diastole measuring 5.2 cm and end systole measuring 4.0 cm) with flattened motion of the intraventricular septum and normal free wall motion. Her ejection fraction by the Simpson method was calculated to be 40%, consistent with mild dilated cardiomyopathy.

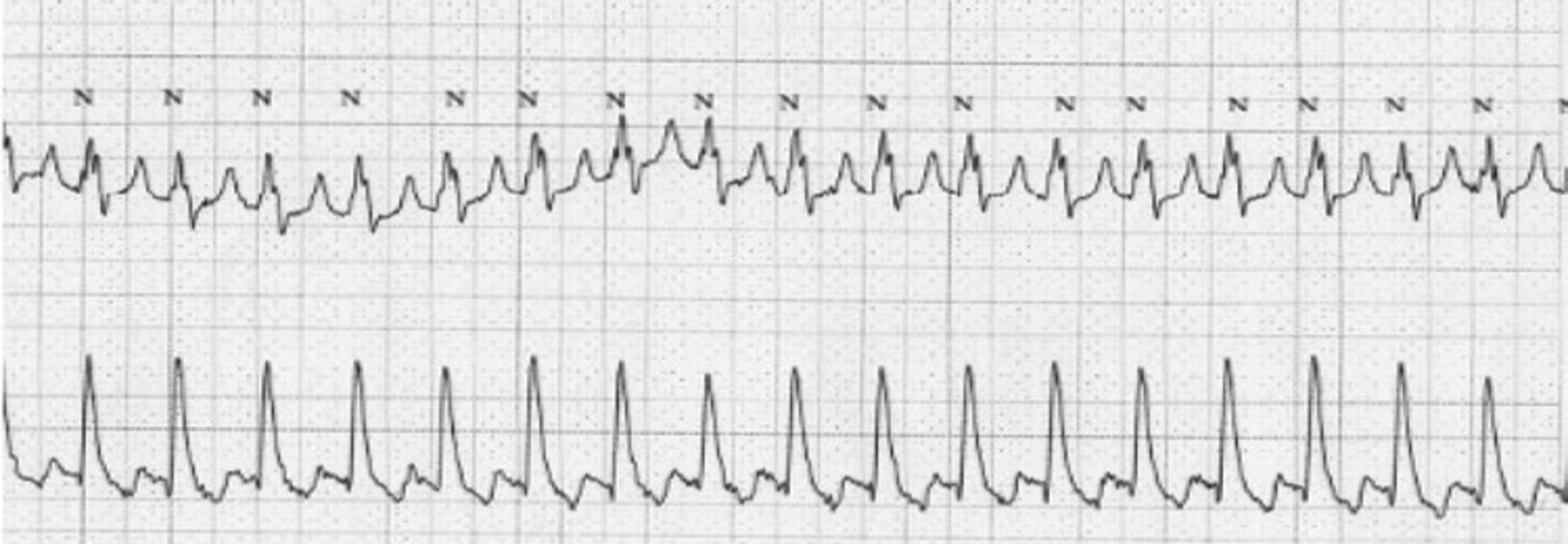
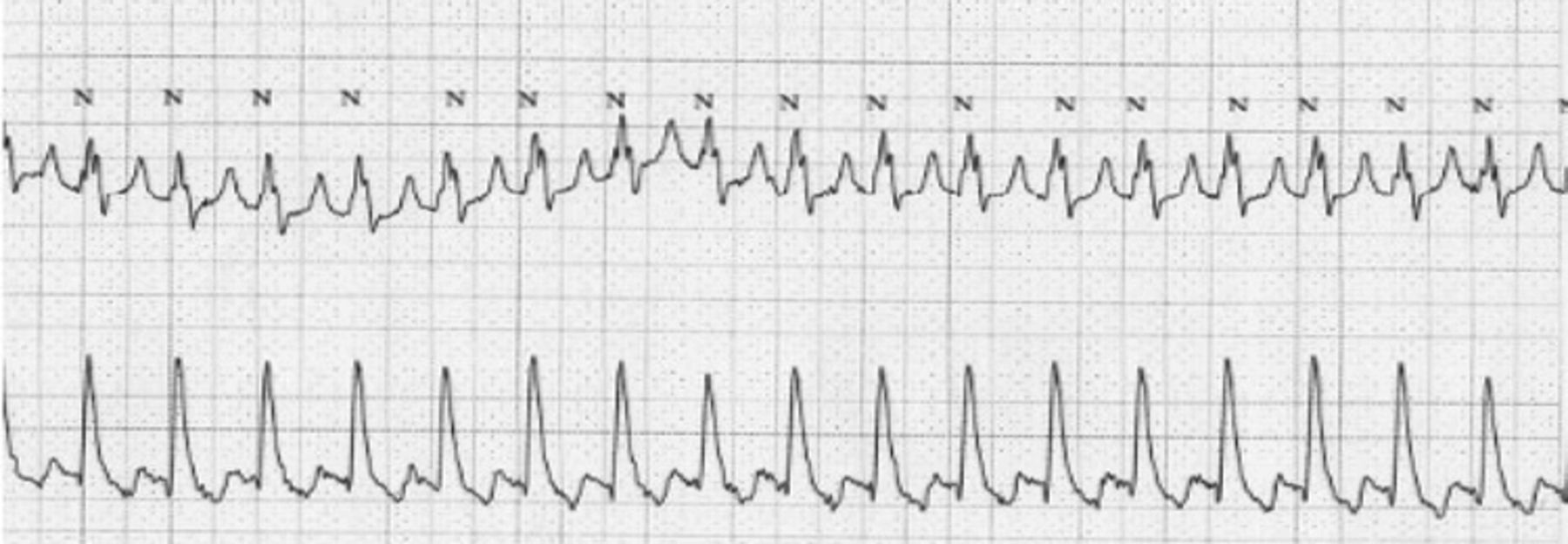
Holter monitoring revealed a wide complex rhythm throughout (Figure 2). Because of this finding, she was referred for an electrophysiology study to determine the etiology of her arrhythmia. Her baseline rhythm was sinus rhythm with a mild prolongation of QRS of 118 milliseconds (Figure 3). During atrial pacing, the patient developed a left bundle-branch block at a paced cycle length of 460 milliseconds (heart rate, 130 beats/min; QRS, 144 milliseconds). During a single atrial extrastimulus protocol at 480/430, her left bundle-branch block pattern recurred, consistent with the effective refractory period of her left bundle branch. Of note, the measurements of her atrium to His potential (60 milliseconds) and her His to ventricle (39 milliseconds) did not change during narrow or wide QRS, again consistent with the effective refractory period of her left bundle branch.

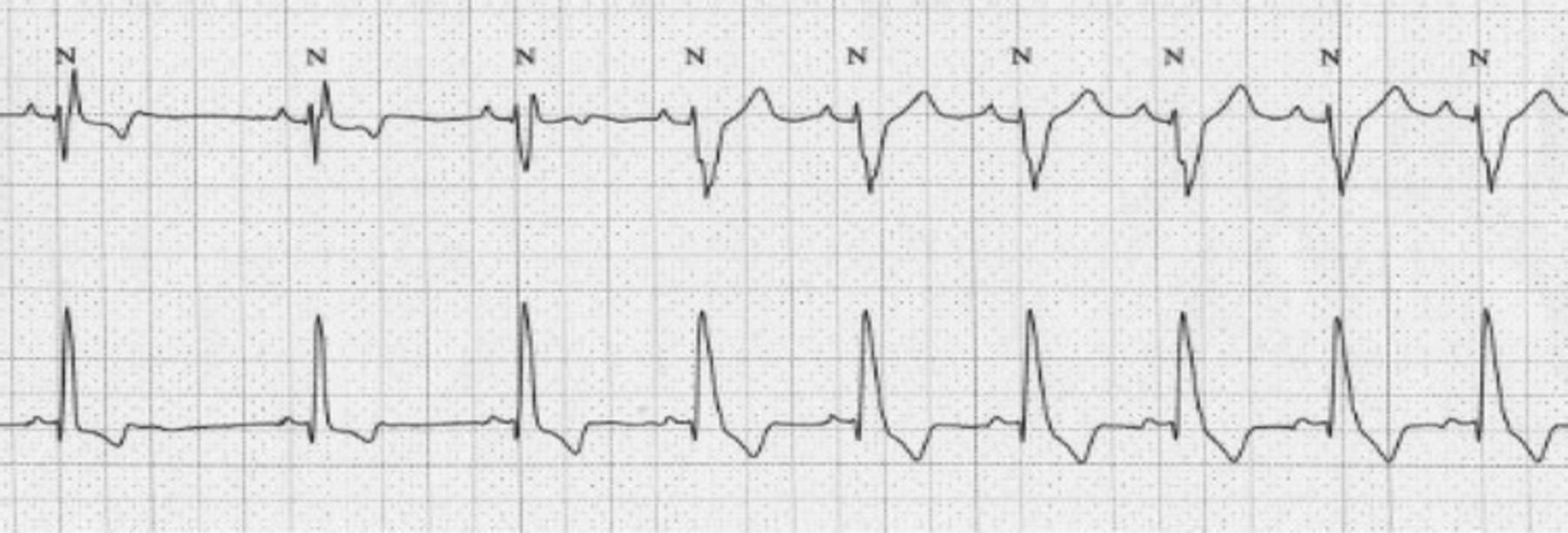
After the electrophysiology study, an exercise stress test showed a baseline electrocardiogram with normal sinus rhythm and an intraventricular conduction delay at a rate of 56 beats/min and a QRS duration of 118 milliseconds. At heart rates exceeding 70 beats/min, she again developed a left bundle-branch block with a QRS duration of 144 milliseconds (Figure 4).
DISCUSSION
Propionic aciduria is a rare condition that on a worldwide basis affects about 1 child per 100,000 births. Mild forms of the disease are probably more common, and the true incidence may be as high as 1 case per 18,000.1 Propionic aciduria is an autosomal recessive organic acidemia due to a defect in propionyl coenzyme A carboxylase, a biotin-dependent enzyme. It leads to defects in the metabolism of valine, isoleucine, methionine, threonine, and odd-chain fatty acids. Associated laboratory findings are anion gap metabolic acidosis, hypoglycemia, ketosis, and hyperammonemia.2
The degree of enzyme deficiency has great prognostic significance. With early onset, patients had a median survival of 0.4 year, while most patients with late onset died before age 4 years. The median age of living early-onset patients was 5.2 years (age range, 1–9.25 years), and the late-onset patients were between 4 and 23 years of age.3 Clinically, neonates are seen with vomiting, poor suck reflex, respiratory distress, hypotonia, and coma.4 As in our patient, another study5 documented that 30% of patients with propionic aciduria were found to have dilated cardiomyopathy with left ventricular dysfunction. The only electrocardiographic abnormality found in the patients in that study was left ventricular hypertrophy.
The effective refractory period denotes the longest coupling interval, or fastest heart rate, that fails to conduct normally over a structure or tissue. In our patient, the effective refractory period was prolonged and did not allow conduction through her Purkinje cell system at slightly increased heart rates (>70 to 100 beats/min). We believe that this rate-dependant left bundle-branch block is due to conduction differences among cells in a “diseased” myocardium, which results in impulse fragmentation and unidirectional conduction block.
To date, a single case report6 exists of a pediatric patient who had latent cardiomyopathy producing exercise-induced left bundle-branch block. In adult patients, exercise-induced left bundle-branch block has been identified at heart rates exceeding 125 beats/min; this finding was associated with coronary perfusion abnormality due to a deficiency in microcirculation or a coronary artery spasm.7,8 A single case report9 exists of exercise-induced left bundle-branch block in an adult with dilated cardiomyopathy.
A left bundle-branch block pattern characterizes the morphologic appearance of the QRS on electrocardiogram. By definition, a left bundle-branch block has a QRS duration of at least 120 milliseconds with a negative deflection in lead V1 and a positive terminal deflection in lead V6.10 In nonpostoperative patients, the underlying cause of rate-dependent bundle-branch block is a prolonged effective refractory period of the specialized conduction tissue involved in the block.
In our patient, a rate-dependent bundle-branch block pattern was initially elicited on a Holter monitor test. She then underwent an electrophysiology study to confirm that no conduction abnormality existed. We believe that her cardiomyopathy secondary to propionic aciduria led to a dilated left ventricle and to an inactive flattened intraventricular septum. As the heart rate increases, her left bundle branch “lags,” producing a left bundle-branch block. We speculate that her left bundle-branch block is due, at least in part, to her propionic aciduria and dilated cardiomyopathy.
In conclusion, our patient's cardiomyopathy is most likely secondary to her propionic aciduria. At this point, we can only postulate that her left bundle-branch block may be caused by propionic aciduria, which results in a prolonged refractory period in her left bundle branch during increased heart rates.
- Academic Division of Ochsner Clinic Foundation
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Cited By...
- No citing articles found.