
Abstract
Obesity prevalence has reached epidemic proportions and is independently associated with numerous cardiovascular disease (CVD) risk factors, including diabetes mellitus, hypertension, dyslipidemia, cancers, sleep apnea, and other major CVDs. Obesity has significant negative impact on CVD, including hypertension, coronary heart disease, heart failure, and arrhythmias via its maladaptive effects on individual CVD risk factors and cardiac structure and function. Despite this negative association between obesity and the incidence and prevalence of CVD, many studies have demonstrated that obese patients with established CVD might have better short- and long-term prognosis, suggesting an “obesity paradox.” This intriguing phenomenon has been well documented in populations with heart failure, coronary heart disease, and hypertension. This review summarizes the adverse effects of obesity on individual CVD risk factors; its role in the genesis of CVDs, including heart failure, coronary heart disease, and hypertension; and the obesity paradox observed in these populations and the potential underlying mechanisms behind this puzzling phenomenon and concludes with a discussion on the potential benefits of weight reduction.
INTRODUCTION
Obesity is a highly prevalent metabolic disorder that is increasing in epidemic proportions in both children and adults in the United States.1–4 With the increasing prevalence of overweight and obesity, they are the second leading cause of preventable death in the United States and soon may overtake cigarette smoking as the leading cause of preventable death.5–7 From the time of the 1988–1994 National Health and Nutrition Examination Survey (NHANES III) to that of the 1999–2000 NHANES survey, the prevalence of overweight and obesity in adults increased from 56% to 65% and 23% to 31%, respectively.4,8 Health care spending associated with obesity-related diseases has increased dramatically and is expected to continue to rise.9 Obesity is associated with numerous comorbidities, such as dyslipidemia, hypertension (HTN), reduced insulin sensitivity, diabetes mellitus, left ventricular (LV) hypertrophy, certain cancers, and sleep apnea/sleep-disordered breathing.2,3,5,6 Obesity is also an independent risk factor for cardiovascular disease (CVD), including HTN, coronary heart disease (CHD), and heart failure (HF) and is associated with an increased risk of morbidity and mortality.6,10–14 Olshansky et al15 noted that the life-shortening effect of obesity could rise, as obese individuals, who are now younger, carry their elevated risk of death into middle and older ages. Besides an altered metabolic profile, a variety of adaptations/alterations in cardiac structure and function occur as adipose tissue accumulates in excess amounts, even in the absence of comorbidities.5
Historically, the Metropolitan Life Insurance Company classification of obesity that has been used was based on body fat as the percentage of ideal body weight,16 but currently overweight and obesity are defined by body mass index (BMI; weight in kilograms/height in meters squared, kg/m2). In adults, overweight is defined as a BMI of 25–29.9 kg/m2; obesity is defined as a BMI≥30 kg/m2. Other less commonly used indices, but possibly with more predictive power, include waist circumference, waist-to-hip ratio, weight-to-height ratio, and body fat.17
OBESITY AND CVD RISK
The prevalence and severity of HTN increase with increasing BMI. Obesity is characterized by various hemodynamic and metabolic abnormalities, including an increase in circulating blood volume and systemic vascular resistance, which contribute to the development of HTN.18–22 Therefore, HTN associated with obesity is characterized by combined volume and pressure overload. Typically, HTN via increased peripheral arterial resistance/afterload leads to ventricular wall thickening without chamber dilatation, which is classified as concentric remodeling or as concentric LV hypertrophy when there is an increase in LV mass.23–26 On the other hand, obesity with elevated circulating blood volume leads to an increase in LV mass via chamber dilatation without a significant increase in wall thickness, a process that is referred to as eccentric LV hypertrophy.9,25 Recently, in a study from our large echocardiographic database,9 we demonstrated the high prevalence of abnormal LV geometric patterns in obese patients. A 10-kg increase in body weight was associated with an increase of 3 and 2.3 mmHg in systolic and diastolic blood pressure, respectively. These increases translated into an estimated 12% increased risk for CHD and 24% increased risk for stroke.27 Also, results from NHANES III indicated that the prevalence of HTN increased progressively with increasing BMI, from 15% at a BMI<25 kg/m2 to 42% at a BMI of 30 kg/m2 in men and from 15% at a BMI<25 kg/m2 to 38% at a BMI of 30 kg/m2 in women.28
The incidence and prevalence of HF and its associated mortality is increasing at alarming rates.10 Despite the progress made in the development of several new therapies in HF management, the overall 5-year mortality rate for HF remains extremely high at nearly 50%.29 Recent epidemiologic evidence from the Framingham Heart Study indicates that overweight and obesity are potent indicators and predictors of subsequent clinical HF.10 In a study of 5,881 participants, Kenchaiah and colleagues10 estimated that the risk of HF increases 5% for men and 7% for women for each increase of 1U in BMI. In fact, a graded increase in the risk of HF was observed across all categories of BMI (Figure 1), suggesting a causal relationship between excess body weight and the development of HF. In a study of 74 morbidly obese patients,30 nearly one-third had clinical evidence of HF, and the probability of HF increased with increasing duration of morbid obesity (Figure 2). At 20 and 25 years of obesity duration, the probability of HF was 66% and 93%, respectively. Obesity typically causes worsening in cardiac relaxation (diastolic dysfunction), which is a common cause of HF.31 Moreover, obesity over a period of time is associated with reduced LV systolic function.32


Obesity is independently associated with the incidence of new CHD cases and adversely affects conventional CHD risk factors, including HTN, diabetes mellitus, dyslipidemia, and the metabolic syndrome.33,34 This negative relationship became more evident as accumulated evidence from long-term follow-up studies found that obesity was associated with CHD, independent of other cardiovascular risk factors.33,34 Data from the Pathobiological Determinants of Atherosclerosis in Youth study35,36 suggest that overweight and obesity in young adults accelerate the progression of atherosclerosis decades before the appearance of clinical manifestations. Prospective studies that reported follow-up data for more than 2 decades, such as the Manitoba Study,37 the Framingham Heart Study,38 and the Harvard School of Public Health Nurses Study,39 have documented that obesity is an independent predictor of clinical CHD. The underlying pathophysiologic mechanisms that might confer an increased risk for CHD include obesity-mediated free fatty acid turnover, induction and promotion of a hypercoagulable and hyperinflammatory state,36,40 an increase in vascular thromboxane receptor gene expression,41 and obesity-mediated reduction in insulin sensitivity.
“OBESITY PARADOX” IN POPULATIONS WITH HF, CHD, AND HTN
Although obesity via its negative impact on systolic and diastolic function predisposes to overt HF, clinical evidence suggests that overweight/obese patients with HF paradoxically seem to have a better clinical prognosis than do their lean counterparts with clinical HF. In essence, obesity is a risk factor for developing HF, but after the onset of HF, obesity is a positive predictor for survival.5,6,10,11,42–49 The existence of this obesity paradox has led physicians to question whether obesity should be treated when associated with HF.
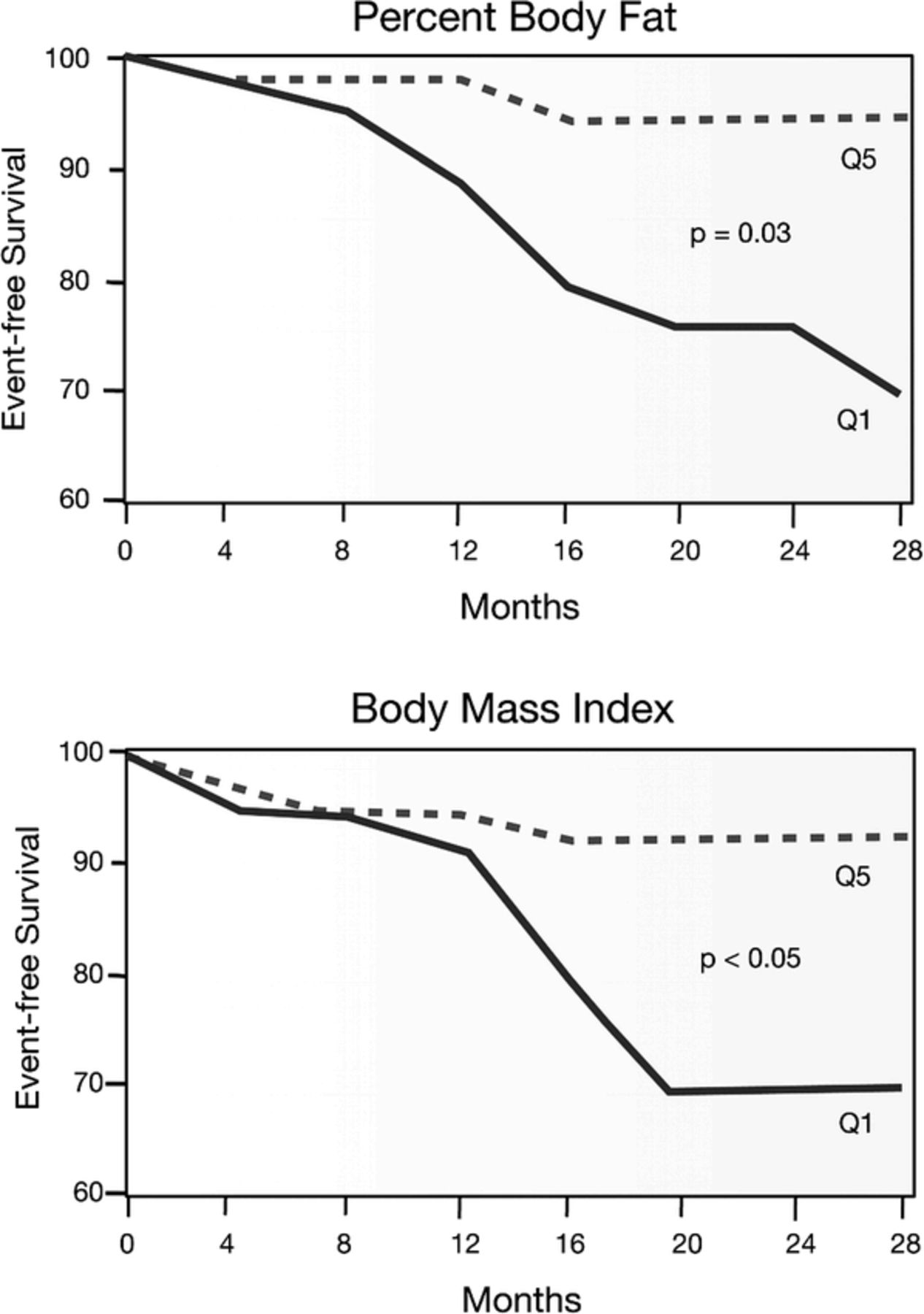
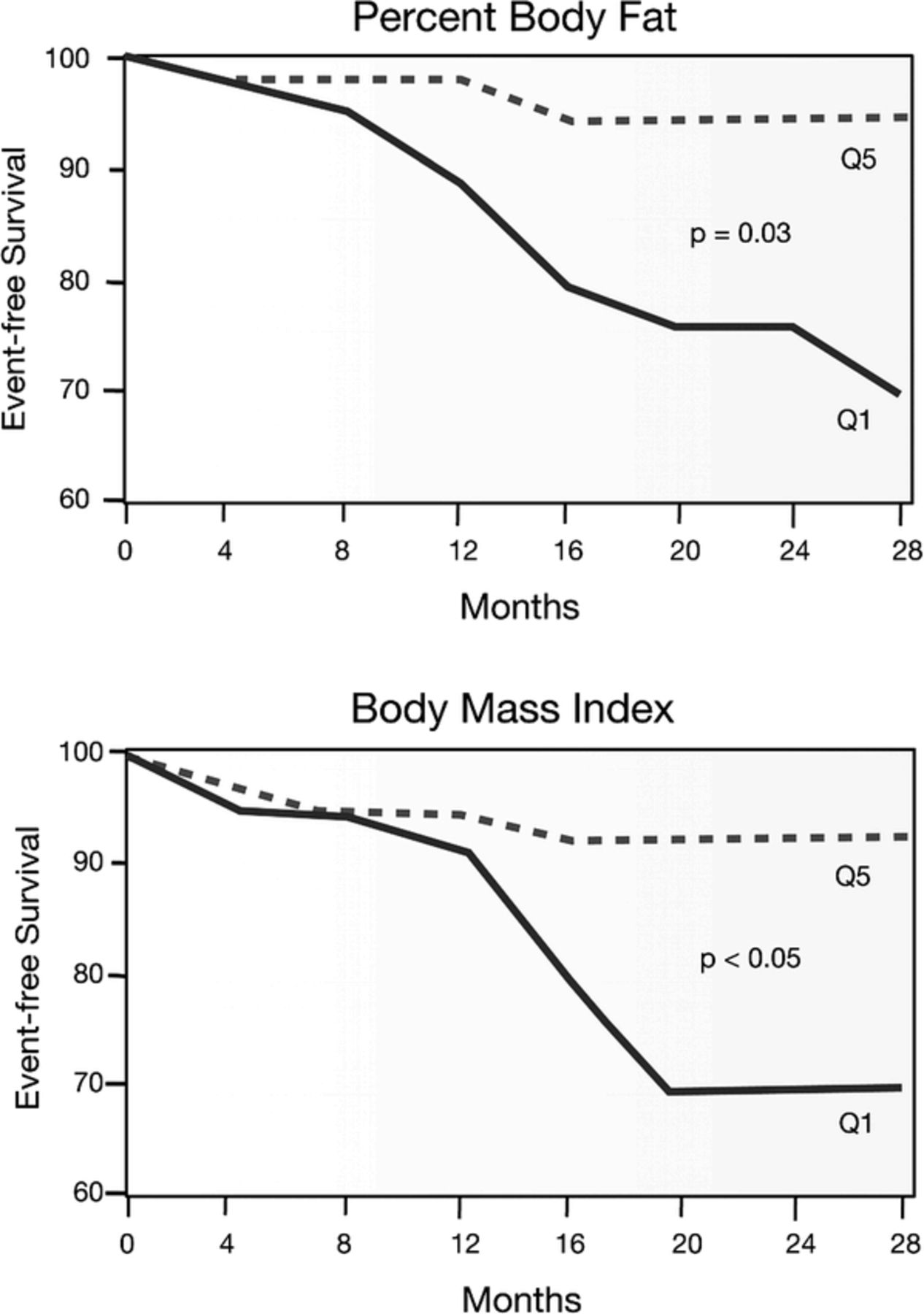
Horwich et al43 studied 1,203 individuals with class IV HF and found that higher BMI was associated with better survival (Figure 3), and multivariate analysis showed an inverse association between BMI and mortality. We recently conducted a study of 209 patients with mostly class II and III HF with a mean ejection fraction of 23% and showed that higher BMI and a higher percentage of body fat were associated with better event-free survival during 2 years of follow-up (Figure 4). In multivariate analysis, both a higher percentage of body fat and higher BMI were independent predictors of event-free survival.44 For every 1% absolute increase in percentage of body fat, we observed a >13% reduction in major clinical events.44 Some investigators have described this as an obesity paradox, whereas others have described the relationship between some of the cardiovascular risk factors and HF prognosis as “reverse epidemiology.”45 Curtis et al46 examined the association between BMI and outcomes in 7,767 stable outpatients with HF from the Digitalis Investigation Group Trial. During 37 months of follow-up, there was a linear decrease in crude all-cause mortality across all BMI groups. In multivariate analysis, overweight and obese patients remained at lower risk for all-cause mortality as compared to normal weight patients. In a preliminary analysis of 875 patients with advanced HF, we looked at the impact of percentage of body fat and BMI on all-cause mortality during 3 years of follow-up. In multivariate analysis, higher percentage of body fat and higher BMI were second only to lower brain natriuretic peptide as independent predictors of better time-dependent survival.42

This phenomenon of obesity paradox is also well described in populations with CHD and HTN, as we mention in the subsequent paragraphs.2,50,51 Despite the negative association between higher BMI and CHD, many studies suggest paradoxically better prognosis in obese patients with CHD and in patients undergoing revascularization (percutaneous intervention, or PCI, and bypass surgery).2,50,51 Recently, in a systematic review of 40 cohort studies including 250,000 patients during 3.8 years of follow-up, Romero-Corral et al51 reported lower total and cardiovascular mortality in overweight and obese patients with CHD as compared to underweight and normal weight individuals. However, in patients with severe obesity (BMI of 35 kg/m2 or greater), excess risk in cardiovascular mortality was noted with no increase in total mortality. These authors concluded that the lack of discriminatory power of BMI to differentiate between body fat and lean mass could have led to better clinical outcomes in overweight and obese patients.51 Another trial examining the glycoprotein IIb/IIIa inhibitor abciximab in patients with unstable angina/non-ST-segment elevation myocardial infarction (NSTEMI) who were not scheduled for coronary intervention showed increased 1-year mortality rates in lower-weight patients compared to normal-weight and obese patients (9.6% in 75-kg group compared with 7.4% and 6.6% in patients with body weight 75–90 kg and >90 kg, respectively; P<.001).52
Buettner and colleagues53 looked at the impact of obesity in 1,676 patients with unstable angina/NSTEMI treated with an early invasive strategy. During 3 years of follow-up, there was almost a linear reduction in all-cause mortality, from 10% in patients with normal BMI to 8% in overweight patients to 4% in obese patients to 0% in severely obese patients with BMI>35 kg/m2. These findings of better prognosis in obese patients with CHD are further supported by encouraging evidence from PCI studies and large registries. Analysis of the Bypass Angioplasty Revascularization Investigation registry,54 including 2,108 patients who underwent PCI and 1,526 patients who underwent coronary artery bypass graft (CABG) surgery, revealed that every unit increase in BMI in the PCI group was associated with 6% lower risk of in-hospital events, including death, myocardial infarction, stroke, and coma. However, in the CABG group, there was no impact of BMI on early in-hospital outcomes. In contrast, higher BMI was associated with worse long-term outcomes in the CABG group but not in the PCI group.54 In a large group of stable patients with CHD who underwent PCI, Gruberg et al55 found better clinical outcomes in overweight and obese patients compared to normal-weight patients despite worse baseline CVD risk profiles. Even postprocedural complications and 1-year mortality rates were lower in overweight and obese patients compared to those in the normal-weight group. Analysis of the New York State Angioplasty database56 that included 95,435 consecutive patients post-PCI during a 4-year period revealed lower in-hospital mortality and major adverse cardiac events in class I (BMI 30–34.9 kg/m2) and class II (BMI 35–39.9 kg/m2) patients compared to normal-weight patients. However, patients at both extremes, underweight (BMI<18.5 kg/m2) and extremely obese (BMI>40 kg/m2) had significantly higher mortality and higher rates of major adverse cardiac events.56
Similarly, studies in populations with HTN have suggested better outcomes and better long-term prognosis in obese patients.2 Recently Uretsky et al57 investigated the effects of obesity on cardiovascular outcomes in 22,576 hypertensive patients with CHD from The International Verapamil SR-Trandolapril Study. At 24 months of follow-up, all-cause mortality was 30% lower in overweight and obese patients, despite less effective blood pressure control in these patients compared to the normal-weight group (Figure 5). A similar relationship was noted in the Systolic Hypertension in the Elderly Study,58 where overweight status was associated with decreased risk of stroke and all-cause mortality as compared to leanness. Almost comparable findings were noted in a younger cohort (aged 30–69 years) with HTN from the Hypertension Detection and Follow-up Program.59 This study showed a U-shaped relationship between all-cause, CVD, and non-CVD mortality and BMI, indicating excess mortality at both extremes of BMI.59 In another study of 800 elderly hypertensive patients randomly assigned to active treatment or placebo, total mortality and CVD and non-CVD major events were highest in those with the leanest BMI quintile.60 The association between BMI and major CVD events was U-shaped, whereas non-CVD mortality decreased with increasing BMI. The BMI level with the lowest risk was 28–29 kg/m2 for total mortality and CVD events, 26–27 kg/m2 for CVD mortality, and 31–32 kg/m2 for non-CVD mortality. In aggregate, these studies suggest that although obesity is a powerful risk factor for HTN and LV hypertrophy, obese hypertensive patients have a better prognosis.60 It has been postulated that lower systemic vascular resistance and lower plasma renin activity in obese hypertensive patients compared to leaner hypertensive patients may partly explain their improved prognosis.10

We also demonstrated this paradoxical association of better prognosis with higher BMI in the referral population for echocardiography. We assessed the impact of LV geometry and obesity on mortality in 30,920 patients with preserved ejection fraction, including 11,792 obese patients as well as 19,128 non-obese patients during an average follow-up of 3.2±1.4 years. Although abnormal LV geometric patterns were more commonly observed in obese versus non-obese patients (49% vs. 44%, P<.0001), all-cause mortality was considerably lower in obese compared to non-obese patients (3.9% vs. 6.5%, P<.0001). In both obese and non-obese patients, there was a progressive increase in mortality with progressive increases in abnormal LV geometry. Although in the entire cohort higher BMI was an independent predictor of better survival, in the obese subgroup higher BMI was associated with higher mortality.9 We also determined the impact of these 2 variables, including LV geometry and obesity, in 8,088 elderly patients (>70 years old) with preserved LV function on all-cause mortality during a 3-year follow-up. Although abnormal LV geometry progressively increased with greater obesity (57%, 59%, and 61%; P<.01 for BMI<25 kg/m2, BMI of 25–30 kg/m2, and BMI≥30 kg/m2, respectively), total mortality was strongly and inversely related with BMI (BMI<18.5 kg/m2, 22% mortality; BMI 18.5–25 kg/m2, 15% mortality; BMI 25–30 kg/m2, 10% mortality; BMI 30–35 kg/m2, 9% mortality; BMI≥35 kg/m2, 8% mortality).61
MECHANISMS FOR THE OBESITY PARADOX
The underlying mechanisms for this apparent obesity paradox remain elusive. It is postulated that lower body weight may be associated with a heightened catabolic state with increasing levels of tumor necrosis factor and other cytokines and imbalance in cortisol/dehydroepiandrosterone ratio.5,6,10 There is evidence from several studies linking adiposity and the natriuretic peptide system; recently, we demonstrated reduced natriuretic peptide levels in obese patients with HF.45,62 This explains the earlier expression of HF with less severe symptoms in the presence of obesity secondary to reduced circulating natriuretic peptide levels. Therefore, obese patients with HF with earlier presentation and less severe symptoms receive more aggressive therapy early on, with better long-term prognosis.45,62
Other lines of evidence suggest enhanced protection against endotoxin/inflammatory cytokines with obesity as well as increased nutritional and metabolic reserves.63–66 Evidence from basic science studies suggests that adipose tissue is occupied with dense soluble tumor necrosis factor α receptors, which have a neutralizing effect on cytokines, including interleukin 1 and tumor necrosis factor α, and might have a protective role in obese patients with acute or chronic HF.67 Also, just being obese with good nutritional and metabolic reserves might confer favorable prognosis in both obese patients with HF and CHD alike.2,5 Obese patients with HF have lower baseline levels of the renin-angiotensin system, which might protect the cardiovascular system from their deleterious effects.68,69 Because obese patients have higher blood pressure levels, they might better tolerate cardioprotective medications and have a better prognosis.63 Nevertheless, despite these potential mechanisms, the exact reasons for these puzzling results remain elusive. In addition, most of these studies have focused on BMI and a few on percentage of body fat, and there is little information regarding other parameters (eg, waist circumference, waist-to-hip ratio) in the obesity paradox.5 Finally, many of the studies did not adjust for smoking and chronic obstructive pulmonary disease among underweight and leaner subjects, as well as nonpurposeful weight loss in the participants, which may suggest worse prognosis for almost every potential etiology.70
WEIGHT LOSS
Studies looking at the impact of weight reduction in overweight and obese cardiac patients have been controversial, some suggesting better clinical outcomes, whereas others indicating no benefits and, in fact, some studies have even suggested detrimental effects. However, other studies assessing mortality based on lean body mass and total body fat content as opposed to BMI showed that losing body fat rather than lean mass has mortality benefits.2,5 In a study of 74 morbidly obese patients, Alpert et al32 showed that significant weight reduction >30% of total body weight with gastroplasty (12 of 14 morbidly obese patients achieved this weight loss) resulted in improvement of New York Heart Association functional class by an average of >1. In this study, weight loss was also associated with marked improvements in LV dimensions and systolic function. MacMahon et al71 demonstrated that even minimal weight loss of 8 kg or 17.6 lb in mildly obese subjects with HTN was associated with significantly greater reductions in LV mass and wall thickness compared to reductions achieved in subjects treated with pharmacologic therapy with β-blockers. Among various nonpharmacologic means of weight reduction, cardiac rehabilitation and exercise training (CRET) is the most extensively studied method; in one particular study from our institution with patients with metabolic syndrome, CRET led to a 37% reduction in the prevalence of metabolic syndrome.72 In a small subgroup of 45 obese patients with CHD from our CRET program, we demonstrated that even small reductions in body weight (>5% or more; average, 10%) was associated with marked improvements in obesity indices, lipids, and exercise capacity when compared to the cohort that did not lose weight.73 Recently, we noted marked reductions in C-reactive protein levels in obese patients with CHD following CRET, whereas lean patients had nonsignificant reductions in C-reactive protein.74 In a preliminary analysis of a much larger sample size, we noted marked improvements in CHD risk factors, including C-reactive protein, lipids, and glucose, among patients with CHD who lost weight; this group had a trend for lower mortality.50 Therefore, these data do not indicate that obesity should be ignored as a risk factor just because an obesity paradox exists. In fact, obesity remains a powerful risk factor for the development of HTN, HF, and CHD, and we believe that purposeful weight reduction should still be emphasized, particularly for the more obese patients with HTN, HF, and CHD, despite the obesity paradox. Additionally, marked weight loss with bariatric surgery has resulted in improved mortality risk, mostly related to diabetes mellitus, cancers, and CVD events.75–77 Although data are limited on the efficacy and safety of these procedures in patients with established CVD, a recent study in 12 patients with severe HF78 suggests safety and improvements in HF prognosis following this surgery that may be considered to be high risk in patients with HF.
CONCLUSIONS
Although obesity is associated with the pathogenesis and progression of CVD, evidence reports the existence of an obesity paradox, in that obese patients with established CVDs appear to have better clinical prognosis. Available evidence supports the benefits of purposeful weight reduction in curbing the obesity pandemic and associated CVDs. Further research is warranted to better understand the puzzling obesity paradox phenomenon, the underlying mechanisms for the obesity paradox, and weight reduction strategies in various subgroups and to better define the optimal weight in these special populations of high-risk patients with and without established CVD to help clinicians guide management in these complicated cases.
- Academic Division of Ochsner Clinic Foundation








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}