
The Mediating Role of Vision in the Relationship between Proprioception and Postural Control in Older Adults, as Compared to Teenagers and Younger and Middle-Aged Adults

 ,
,  , ,
, ,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Procedure
2.4. Proprioception
2.5. Postural Control
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Aman, J.E.; Elangovan, N.; Yeh, I.; Konczak, J. The effectiveness of proprioceptive training for improving motor function: A systematic review. Front. Hum. Neurosci. 2015, 8, 1075. [Google Scholar] [CrossRef] [Green Version]
- Ansorge, U.; Francis, G.; Herzog, M.H.; Öğmen, H. Visual masking and the dynamics of human perception, cognition, and consciousness A century of progress, a contemporary synthesis, and future directions. Adv. Cogn. Psychol. 2007, 3, 1. [Google Scholar] [CrossRef]
- Ashton-Miller, J.A.; Wojtys, E.M.; Huston, L.J.; Fry-Welch, D. Can proprioception really be improved by exercises? Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 128–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delmas, S.; Watanabe, T.; Yacoubi, B.; Christou, E.A. Age-associated increase in postural variability relate to greater low-frequency center of pressure oscillations. Gait Posture 2021, 85, 103–109. [Google Scholar] [CrossRef]
- Doumas, M.; Smolders, C.; Krampe, R.T. Task prioritization in aging: Effects of sensory information on concurrent posture and memory performance. Exp. Brain Res. 2008, 187, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Felson, D.T.; Gross, K.D.; Nevitt, M.C.; Yang, M.; Lane, N.E.; Torner, J.C.; Lewis, C.E.; Hurley, M.V. The effects of impaired joint position sense on the development and progression of pain and structural damage in knee osteoarthritis. Arthritis Care Res. 2009, 61, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Gaerlan, M.G. The Role of Visual, Vestibular, and Somatosensory Systems in Postural Balance. Master’s Thesis, University of Nevada Las Vegas, Las Vegas, NV, USA, 2010. [Google Scholar]
- Ghai, S.; Driller, M.; Ghai, I. Effects of joint stabilizers on proprioception and stability: A systematic review and meta-analysis. Phys. Ther. Sport 2016, 25, 65–75. [Google Scholar] [CrossRef]
- Gilman, S. Joint position sense and vibration sense: Anatomical organisation and assessment. J. Neurol. Neurosurg. Psychiatry 2002, 73, 473–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goble, D.J.; Coxon, J.P.; Wenderoth, N.; Van Impe, A.; Swinnen, S.P. Proprioceptive sensibility in the elderly: Degeneration, functional consequences and plastic-adaptive processes. Neurosci. Biobehav. Rev. 2009, 33, 271–278. [Google Scholar] [CrossRef]
- Goldstone, A.; Mayhew, S.D.; Hale, J.R.; Wilson, R.S.; Bagshaw, A.P. Thalamic functional connectivity and its association with behavioral performance in older age. Brain Behav. 2018, 8, e00943. [Google Scholar] [CrossRef]
- Gomez-Bruton, A.; Navarrete-Villanueva, D.; Pérez-Gómez, J.; Vila-Maldonado, S.; Gesteiro, E.; Gusi, N.; Villa-Vicente, J.G.; Espino, L.; Gonzalez-Gross, M.; Casajus, J.A.; et al. The effects of age, organized physical activity and sedentarism on fitness in older adults: An 8-year longitudinal study. Int. J. Environ. Res. Public Health 2020, 17, 4312. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.; Tremblay, L. Using proprioception to control ongoing actions: Dominance of vision or altered proprioceptive weighing? Exp. Brain Res. 2018, 236, 1897–1910. [Google Scholar] [CrossRef] [PubMed]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A study of concurrent and construct validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef]
- Hallal, P.C.; Victora, C.G. Reliability and validity of the international physical activity questionnaire (IPAQ). Med. Sci. Sports Exerc. 2004, 36, 556. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Anson, J.; Waddington, G.; Adams, R.; Liu, Y. The role of ankle proprioception for balance control in relation to sports performance and injury. BioMed Res. Int. 2015, 2015, 842804. [Google Scholar] [CrossRef] [Green Version]
- Heuninckx, S.; Wenderoth, N.; Swinnen, S.P. Age-related reduction in the differential pathways involved in internal and external movement generation. Neurobiol. Aging 2010, 31, 301–314. [Google Scholar] [CrossRef]
- Heuninckx, S.; Wenderoth, N.; Swinnen, S.P. Systems neuroplasticity in the aging brain: Recruiting additional neural resources for successful motor performance in elderly persons. J. Neurosci. 2008, 28, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Hurler, M.V.; Rees, J.; Newham, D.J. Quadriceps function, proprioceptive acuity and functional performance in healthy young, middle-aged and elderly subjects. Age Ageing 1998, 27, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Jo, H.J.; Song, A.Y.; Lee, K.J.; Lee, D.C.; Kim, Y.H.; Sung, P.S. A kinematic analysis of relative stability of the lower extremities between subjects with and without chronic low back pain. Eur. Spine J. 2011, 20, 1297–1303. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.-H.; Lee, J.-H.; Ahn, S.-E.; Park, M.-J. Effect of time after anterior cruciate ligament tears on proprioception and postural stability. PLoS ONE 2015, 10, e0139038. [Google Scholar] [CrossRef] [Green Version]
- Lima, L.V.; Abner, T.S.S.; Sluka, K.A. Does exercise increase or decrease pain? Central mechanisms underlying these two phenomena. J. Physiol. 2017, 595, 4141–4150. [Google Scholar] [CrossRef] [Green Version]
- Lord, S.R.; Clark, R.D.; Webster, I.W. Postural stability and associated physiological factors in a population of aged persons. J. Gerontol. 1991, 46, M69–M76. [Google Scholar] [CrossRef]
- MacKinnon, C.D. Sensorimotor anatomy of gait, balance, and falls. In Handbook of Clinical Neurology; Elsevier BV: Amsterdam, The Netherlands, 2018; pp. 3–26. [Google Scholar] [CrossRef]
- McCaskey, M.A.; Schuster-Amft, C.; Wirth, B.; de Bruin, E.D. Effects of proprioceptive exercises on pain and function in chronic neck-and low back pain rehabilitation: A systematic literature review. Physiotherapy 2015, 101, e969–e970. [Google Scholar] [CrossRef] [Green Version]
- McChesney, J.W.; Woollacott, M.H. The effect of age-related declines in proprioception and total knee replacement on postural control. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2000, 55, M658–M666. [Google Scholar] [CrossRef] [Green Version]
- Melián-Ortiz, A.; Varillas-Delgado, D.; Laguarta-Val, S.; Rodríguez-Aparicio, I.; Senent-Sansegundo, N.; Fernández-García, M.; Roger-de Oña, I. Reliability and concurrent validity of the app Goniometer Pro vs. Universal Goniometer in the determination of passive knee flexion. Acta Ortop. Mex. 2019, 33, 18–23. [Google Scholar]
- Michaelidis, M.; Koumantakis, G.A. Effects of knee injury primary prevention programs on anterior cruciate ligament injury rates in female athletes in different sports: A systematic review. Phys. Ther. Sport 2014, 15, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Mourcou, Q.; Fleury, A.; Diot, B.; Vuillerme, N. iProprio: A Smartphone-based system to measure and improve proprioceptive function. In Proceedings of the 2016 IEEE 38th Annual International Conference of The Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 2622–2625. [Google Scholar]
- Nagano, Y.; Ishida, K.; Tani, T.; Kawasaki, M.; Ikeuchi, M. Short and long-term effects of exergaming for the elderly. Springerplus 2016, 5, 793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, D.A. Kinesiology of the Musculoskeletal System-E-Book: Foundations for Rehabilitation; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Newcomer, K.; Laskowski, E.R.; Yu, B.; Larson, D.R.; An, K.-N. Repositioning error in low back pain: Comparing trunk repositioning error in subjects with chronic low back pain and control subjects. Spine 2000, 25, 245. [Google Scholar] [CrossRef] [PubMed]
- Noé, F.; Amarantini, D.; Paillard, T. How experienced alpine-skiers cope with restrictions of ankle degrees-of-freedom when wearing ski-boots in postural exercises. J. Electromyogr. Kinesiol. 2009, 19, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Noé, F.; García-Massó, X.; Delaygue, P.; Melon, A.; Paillard, T. The influence of wearing ski-boots with different rigidity characteristics on postural control. Sports Biomech. 2018, 19, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Noé, F.; Paillard, T. Is postural control affected by expertise in alpine skiing? Br. J. Sports Med. 2005, 39, 835–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.H.; Mancini, M.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B. Quantifying effects of age on balance and gait with inertial sensors in community-dwelling healthy adults. Exp. Gerontol. 2016, 85, 48–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Sousa, M.Á.; del Pozo-Cruz, J.; Olivares, P.R.; Cano-Gutiérrez, C.A.; Izquierdo, M.; Ramírez-Vélez, R. Role for Physical Fitness in the Association between Age and Cognitive Function in Older Adults: A Mediation Analysis of the SABE Colombia Study. Int. J. Environ. Res. Public Health 2021, 18, 751. [Google Scholar] [CrossRef] [PubMed]
- Pérez, M.R.; Rodríguez, C.R.; González, J.G.P. Revisión narrativa y desarrollo de un programa de intervención para la disminución de los efectos del Alzheimer a través de la práctica del Surf en Personas Mayores (Narrative review and development of an intervention program for reducing Alzheimer’s eff. Retos 2017, 32, 106–110. [Google Scholar] [CrossRef]
- Petrella, R.J.; Lattanzio, P.J.; Nelson, M.G. Effect of age and activity on knee joint proprioception. Am. J. Phys. Med. Rehabil. 1997, 76, 235–241. [Google Scholar] [CrossRef]
- Piirtola, M.; Era, P. Force platform measurements as predictors of falls among older people—A review. Gerontology 2006, 52, 1–16. [Google Scholar] [CrossRef]
- Prado, J.M.; Stoffregen, T.A.; Duarte, M. Postural sway during dual tasks in young and elderly adults. Gerontology 2006, 53, 274–281. [Google Scholar] [CrossRef]
- Quijoux, F.; Vienne-Jumeau, A.; Bertin-Hugault, F.; Zawieja, P.; Lefèvre, M.; Vidal, P.P.; Ricard, D. Center of pressure displacement characteristics differentiate fall risk in older people: A systematic review with meta-analysis. Ageing Res. Rev. 2020, 62, 101117. [Google Scholar] [CrossRef]
- Riva, D.; Bianchi, R.; Rocca, F.; Mamo, C. Proprioceptive Training and Injury Prevention in a Professional Men’s Basketball Team: A Six-Year Prospective Study. J. Strength Con. Res. 2016, 30, 461–475. [Google Scholar] [CrossRef] [Green Version]
- Sherrington, C.S. Yale University Mrs. Hepsa Ely Silliman Memorial Lectures. The Integrative Action of the Nervous System; Yale University Press: New Haven, CT, USA, 1906. [Google Scholar] [CrossRef]
- Solana-Tramunt, M. Entrenament de la Propiocepció Conscient de la Columna Vertebral Lumbar: Una Aplicació a La Natació Subaquàtica. Ph.D. Thesis, Universitat Ramon Llull, Barcelona, Spain, 2011; 316p. [Google Scholar]
- Sun, F.; Norman, I.J.; While, A.E. Physical activity in older people: A systematic review. BMC Public Health 2013, 13, 449. [Google Scholar] [CrossRef] [Green Version]
- Suner-Keklik, S.; Cobanoglu-Seven, G.; Kafa, N.; Ugurlu, M.; Guzel, N.A. The validity and reliability of knee proprioception measurement performed with inclinometer in different positions. J. Sport Rehabil. 2017, 26, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Vaillant, J.; Coisne, A.; Dumolard, A. Alteration of neck proprioceptive capacity in women with fibromyalgia. Ann. Phys. Rehabil. Med. 2017, 60, e18. [Google Scholar] [CrossRef]
- Van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; van Cingel, R.E.H. How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12, e0189876. [Google Scholar] [CrossRef] [Green Version]
- Vanmeerhaeghe, A.F.; Rodriguez, D.R.; Tutusaus, L.C.; Calafat, C.B.; Riera, M.L.; Vidal, A.M. Diferencias en la estabilidad postural estática y dinámica según sexo y pierna dominante. Apunts. Med. l’Esport 2009, 44, 74–81. [Google Scholar] [CrossRef]
- Vaugoyeau, M.; Viel, S.; Amblard, B.; Azulay, J.P.; Assaiante, C. Proprioceptive contribution of postural control as assessed from very slow oscillations of the support in healthy humans. Gait Posture 2008, 27, 294–302. [Google Scholar] [CrossRef]
- Verkhoshansky, Y. Main features of a modern scientific sports training theory. New Stud. Athl. 1998, 13, 9–20. [Google Scholar]
- Vieira, E.R.; Palmer, R.C.; Chaves, P.H.M. Prevention of falls in older people living in the community. BMJ 2016, 353, i1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viel, S.; Vaugoyeau, M.; Assaiante, C. Adolescence: A transient period of proprioceptive neglect in sensory integration of postural control. Mot. Control 2009, 13, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Waddington, G.S.; Adams, R.D. The Effect of a 5-Week Wobble-Board Exercise Intervention on Ability to Discriminate Different Degrees of Ankle Inversion, Barefoot and Wearing Shoes: A Study in Healthy Elderly. J. Am. Geriatr. Soc. 2004, 52, 573–576. [Google Scholar] [CrossRef]
- Wang, H.; Ji, Z.; Jiang, G.; Liu, W.; Jiao, X. Correlation among proprioception, muscle strength, and balance. J. Phys. Ther. Sci. 2016, 28, 3468–3472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.M.; Davids, K.; Williams, J.G.P. Visual Perception and Action in Sport; Taylor & Francis: Abingdon, UK, 1999. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | n | Age (Years) | Weight (Kg) | Body Mass Index (Kg/m2) | Physical Activity Level (METS) |
|---|---|---|---|---|---|
| Teenagers | 30 | 14.4 ± 1.7 | 58.1 ± 11.1 | 21.0 ± 3.0 | 3320.9 ± 1204.6 |
| Young adults | 29 | 23.6 ± 2.7 | 62.2 ± 9.7 | 22.1 ± 2.2 | 4219.0 ± 1824.2 |
| Middle-aged adults | 30 | 45.4 ± 6.7 | 68.5 ± 24.6 | 23.9 ± 3.7 | 6976.3 ± 2898.0 |
| Older adults | 30 | 73.5 ± 5.9 | 65.8 ± 7.1 | 25.8 ± 2.4 | 3927.8 ± 1569.3 |
| MVAP ROE | MVML ROE | Área Total ROE | MVAP RCE | MVML RCE | Total Area RCE | |
|---|---|---|---|---|---|---|
| MVML ROE | 0.79 * | — | ||||
| Area total ROE | 0.74 * | 0.80 * | — | |||
| MVAP RCE | 0.78 * | 0.63 * | 0.55 * | — | ||
| MVML RCE | 0.70 * | 0.81 * | 0.63 * | 0.79 * | — | |
| Total Area RCE | 0.65 * | 0.67 * | 0.72 * | 0.72 * | 0.82 * | — |
| Propioception | −0.06 | 0.01 | 0.05 | 0.09 | 0.09 | 0.03 |
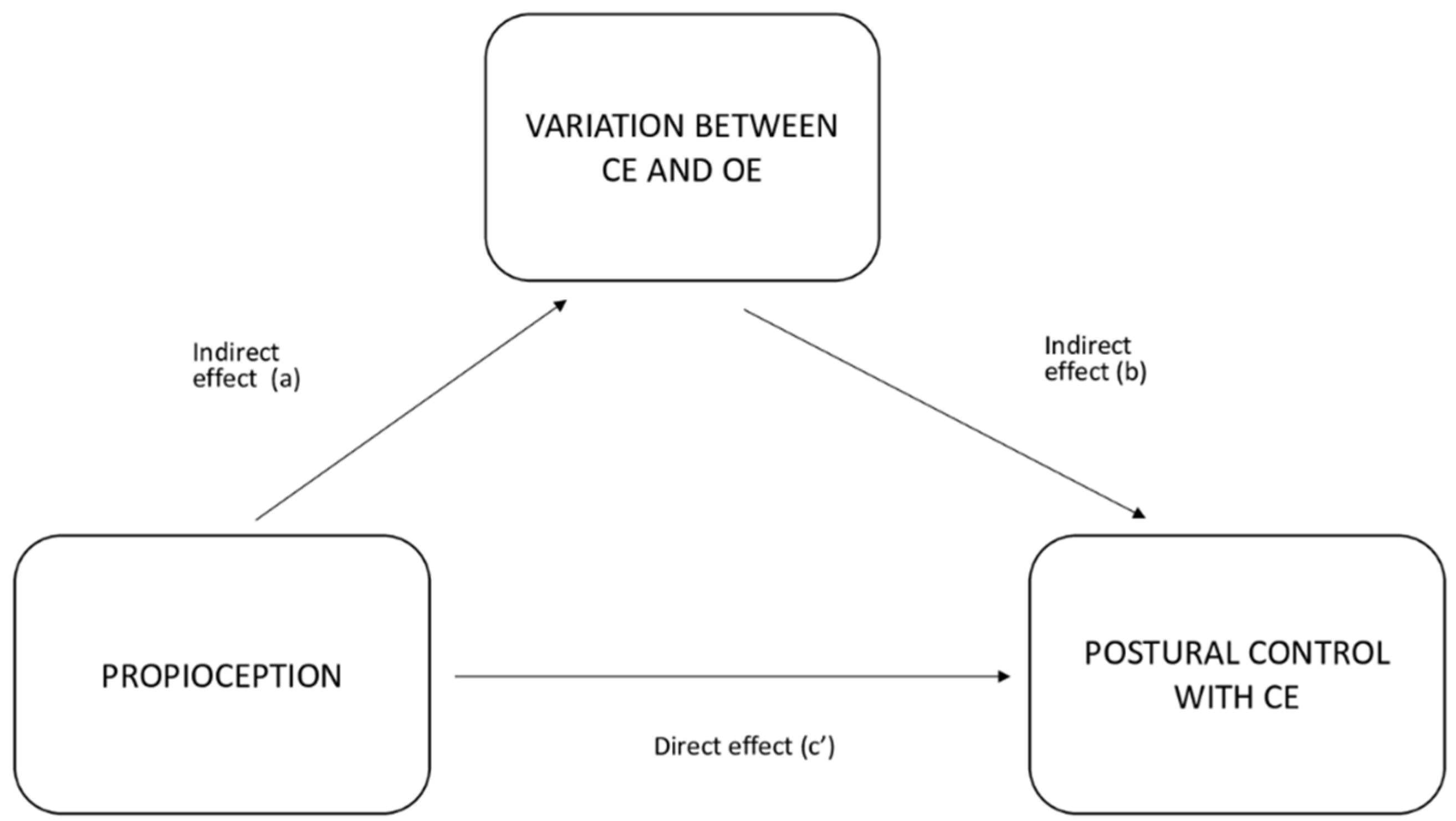
| Postural Control Variable | Effect | Coefficient | Confidence Interval | t | p-Value | % Mediation |
|---|---|---|---|---|---|---|
| MVAP | Indirect (a × b) | 0.070 | 0.008; 0.132 | 2.223 | 0.026 * | 88.1 |
| Direct (c) | 0.009 | −0.147; 0.167 | 0.118 | 0.906 | 11.9 | |
| Total (c + a × b) | 0.079 | −0.078; 0.238 | 0.988 | 0.323 | 100.0 | |
| MVML | Indirect (a × b) | 0.045 | 0.002; 0.089 | 2.050 | 0.040 * | 74.1 |
| Direct (c) | 0.016 | −0.103; 0.135 | 0.263 | 0.792 | 25.9 | |
| Total (c + a × b) | 0.061 | −0.058; 0.182 | 1.009 | 0.313 | 100.0 | |
| Total Area | Indirect (a × b) | −2.12 | −6.73; 2.49 | −0.902 | 0.367 | 34.5 |
| Direct (c) | 4.04 | −9.19; 17.26 | 0.598 | 0.550 | 65.5 | |
| Total (c + a × b) | 1.92 | −12.00; 15.83 | 0.270 | 0.787 | 100.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nieto-Guisado, A.; Solana-Tramunt, M.; Marco-Ahulló, A.; Sevilla-Sánchez, M.; Cabrejas, C.; Campos-Rius, J.; Morales, J. The Mediating Role of Vision in the Relationship between Proprioception and Postural Control in Older Adults, as Compared to Teenagers and Younger and Middle-Aged Adults. Healthcare 2022, 10, 103. https://doi.org/10.3390/healthcare10010103
Nieto-Guisado A, Solana-Tramunt M, Marco-Ahulló A, Sevilla-Sánchez M, Cabrejas C, Campos-Rius J, Morales J. The Mediating Role of Vision in the Relationship between Proprioception and Postural Control in Older Adults, as Compared to Teenagers and Younger and Middle-Aged Adults. Healthcare. 2022; 10(1):103. https://doi.org/10.3390/healthcare10010103
Chicago/Turabian StyleNieto-Guisado, Ainhoa, Monica Solana-Tramunt, Adrià Marco-Ahulló, Marta Sevilla-Sánchez, Cristina Cabrejas, Josep Campos-Rius, and Jose Morales. 2022. "The Mediating Role of Vision in the Relationship between Proprioception and Postural Control in Older Adults, as Compared to Teenagers and Younger and Middle-Aged Adults" Healthcare 10, no. 1: 103. https://doi.org/10.3390/healthcare10010103