Article Text

Abstract
Background: A weak or disrupted internal anal sphincter can cause passive faecal incontinence. Conservative measures may help some patients but there is no simple surgical solution for those who fail conservative treatment. A successful technique using trans-sphincteric injection of a bulking agent to augment the internal anal sphincter was developed in a previous pilot study.
Aim: To determine the clinical results and underlying physiological effects of biomaterial injection.
Patients: Six patients (four males, median age 53 years (range 36–65)) with faecal incontinence to solid or liquid stool related to poor internal anal sphincter function, of varied aetiology, were recruited.
Methods: Silicone based biomaterial injections were performed, under local anaesthesia, with antibiotic cover. Three injections were placed circumferentially, trans-sphincterically, entering away from the anal margin and injecting at or just above the dentate line. Anorectal physiological studies, endoanal ultrasound, a bowel symptom diary, a validated incontinence score, and quality of life questionnaires were completed before treatment and on completion of follow up.
Results: At a median follow up of 18 months (range 15–19), five of six patients had marked symptom improvement. Faecal incontinence scores improved from a median of 14/24 (range 11–20) before to 8/24 (6–15) after injection. Short form-36 quality of life physical and social function scores improved from a median of 26/100 (5–33) to 79/100 (25–100) and from 10/100 (5–37) to 100/100 (50–100), respectively. There was a corresponding physiological increase in maximum anal resting and squeeze pressures. Ultrasound showed the Bioplastique to be retained in the correct position in the improved patients without migration. There were no complications.
Conclusion: Trans-sphincteric injection of silicone biomaterial can provide a marked improvement in faecal incontinence related to a weak or disrupted internal anal sphincter. This is associated with improved sphincter function and quality of life.
- faecal incontinence
- internal anal sphincter dysfunction
- biomaterial injection
- IAS, internal anal sphincter
- PVP, polyvinylpyrrolidone
- SF-36, short form-36
Statistics from Altmetric.com
The internal anal sphincter (IAS) provides most of the resting anal tone1 and is the main muscle responsible for the prevention of faecal leakage.2 A structurally intact but weak IAS can be commonly due to primary idiopathic degeneration,3 or secondary to other tissue disorders such as scleroderma.4 The IAS can also be damaged, most commonly at childbirth or during anal surgery. While some patients with symptomatic incontinence due to IAS degeneration or disruption are helped by antidiarrhoeal treatments such as loperamide or codeine, many are not and the benefit may be only temporary.
Direct surgical repair of the IAS, which is normally only 2.4–3.4 mm thick5 and held at a constant basal tension, has been attempted but has not proved beneficial in the long term.6,7 Other more complex surgical interventions, such as a dynamic graciloplasty or implantation of an artificial bowel sphincter, can give good results but are associated with a high complication and failure rate.8,9 Island anoplasty may be of some benefit where there is an identifiable sphincter defect but there is a high rate of wound breakdown.7 Sacral nerve stimulation is a less invasive procedure with a lower complication rate but experience is still limited.10
An alternative approach to IAS deficiency is to inject a bulking agent either around the IAS or into a defect in the IAS to enhance its function. This has been reported previously in four uncontrolled studies with varying results. In the first, autologous fat was injected perianally and several injections were required.11 The second was a single case report of autologous fat injection after obstetric related IAS damage.12 These showed a short term improvement in symptoms that decreased with time and required repeated injections due to migration and absorption of the injected material. The third used polytetrafluoroethylene paste injected in 11 patients,13 seven of whom had incontinence following internal sphincterotomy. Again, there was a similar improvement in continence in these patients. The fourth involved injection of glutaraldehyde cross linked collagen around the IAS, improving symptoms in 65% of patients.14
Silicone injections (Macroplastique; Uroplasty Ltd, Reading, UK) have been used in the treatment of urinary stress incontinence to augment the bladder neck and increase urethral resistance.15 In a pilot study performed in our institution, a technique for intrasphincteric silicone injection (Bioplastique; Uroplasty Ltd) was developed for faecal incontinence.16 After initial difficulties with infection of the injected material, post-injection pain, and leakage along the needle track, the technique was refined. This study reports the medium term clinical results of patients treated for faecal incontinence due to IAS deficiency with silicone Bioplastique injections using this refined technique and the corresponding physiological changes in anal sphincter function.
METHODS
Patients with severe passive faecal incontinence for solid or liquid stool, due to IAS dysfunction, were selected for injection with Bioplastique. Patients with IAS muscle degeneration and those with discrete IAS defects were included. All patients had failed standard conventional treatment including antidiarrhoeal agents and behavioural therapy (biofeedback), and were considered psychologically suitable to enter a trial. Patients with perianal sepsis, severe scarring, diabetes, immunosupression, or those who were pregnant were excluded. Table 1⇓ shows patient details.
Characteristics of the patients treated with Bioplastique injections
Bioplastique is an injectable material that consists of textured polydimethylsiloxane particles suspended in a bioexcretable carrier hydrogel of polyvinylpyrrolidone (povidone, PVP). Prior to the injections, patients underwent anorectal physiological testing17 to assess sphincter function and an endoanal ultrasound18 to assess sphincter structure. Anal manometry was performed using a pull through technique with an eight channel water perfused system (MMS, Enschede, Holland). The maximum anal resting pressure, and maximum squeeze pressure (the increment above resting pressure) were recorded. Rectal sensation to balloon distension with air at threshold, urge, and maximum tolerated volume was recorded. In addition, a two week bowel symptom diary, validated faecal incontinence severity score,19 and the short form-36 (SF-36) health survey questionnaire20 were completed. These were repeated after completion of follow up.
The injections were performed under local anaesthesia as an outpatient procedure. The patient was placed in the prone jack-knife position and the area cleaned, including anal canal irrigation with betadine solution. Under thorough local anaesthesia, the 18 gauge 2.5 inch needle entered the skin about 1 inch from the anal margin. It was tracked trans-sphincterically to the IAS at the level of, or slightly above, the dentate line, being guided by an anally placed digit. Care was taken not to penetrate the anal mucosa. Three injections of 2 ml of bioplastique were injected at the 3, 7, and 11 o'clock positions, into the area of the internal anal sphincter. This corresponds to the anatomical location of the physiological anal cushions within the anal canal, and was intended to augment the effect of these cushions. This amount of biomaterial had previously been shown to be effective.16
Ultrasound guidance was considered, as the technique was previously developed. However, real time accurate needle guidance proved to be difficult. Post-procedural ultrasound was not performed until six weeks after injection to avoid possible compression or displacement of the biomaterial.
Prior to injection the patient was given intravenous prophylactic antibiotics (gentamicin 160 mg and metronidazole 500 mg). The patient was observed for a four hour period post-procedure to exclude early complications of pain and bleeding or any other unexpected complications. They were then discharged with post-procedural oral antibiotics (cephalexin 500 mg four times daily, metronidazole 400 mg three times daily), analgesia, and laxatives for one week.
In view of the small numbers, the results are presented in full but limited statistical analysis was performed using the Wilcoxon paired samples test.
The Harrow Research Ethics Committee granted the study ethics approval and all patients gave informed consent.
RESULTS
Six patients (four males), median age 53 years (range 36–65), were injected and the median follow up was 18 months (range 15–19). There was a marked improvement in symptoms and patient satisfaction in five of six patients. The patient who did not improve (patient No 2) proceeded to have a colostomy formed.
Faecal incontinence scores (worst score=24, best score=0) improved significantly from a median of 14 (range 11–20) before the procedure to 8 (range 6–15) after the procedure (p=0.04). There was a significant improvement in the quality of life scores, as shown by the change in the SF-36 scores (worst score=0, best score=100). The physical function score improved from a median of 26 (range 5–33) pre-procedure to 79 (range 25–100) post-procedure (p=0.02) and social function score from 10 (range 5–37) to 100 (range 50–100) (p=0.02) (table 2⇓).
Continence scores, quality of life scores, and anal manometry before and after injection
Median resting anal pressure showed a significant increase from 46 cm H2O (range 20–79) to 75 cm H2O (range 57–96) (p=0.03) and median squeeze pressure increased from 98 cm H2O (range 63–268) to 142 cm H2O (range 57–300) (p=0.1) (table 2⇑).
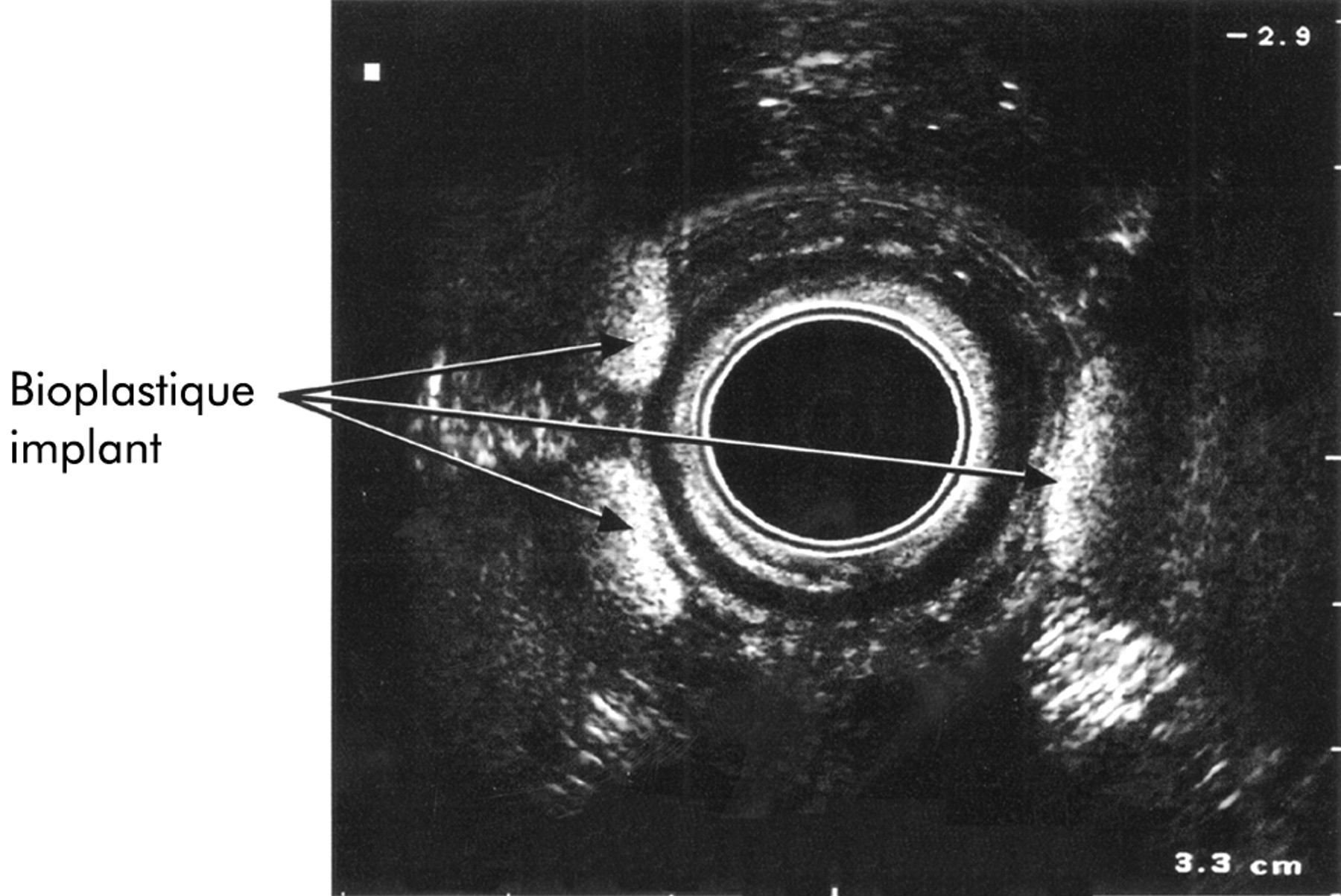
Endoanal ultrasound scans in the five patients who showed a marked improvement confirmed that the Bioplastique was within the upper part of the anal canal extending up to, and partly beyond, the level of the puborectalis ring (see fig 1⇓). The material remained at the site of injection with no apparent local migration, either within or around the IAS. In the patient who showed no improvement, ultrasound revealed that the residual Bioplastique had migrated to lie above the puborectalis muscle so that there was no material remaining within the anal canal.
{kind=link}
Endoanal ultrasound showing injected Bioplastique at three circumferential sites in a patient with idiopathic degeneration.
There were no episodes of infection or leakage in any of the six patients. No patient experienced severe pain or constipation, and erosion of the implants was not encountered.
DISCUSSION
This study has shown that it is possible to treat patients with severe resistant passive faecal incontinence due to IAS weakness or disruption with an injectable biomaterial producing good medium term clinical results.
This series was on a relatively small number of patients. This reflects the fact that passive faecal incontinence, due to IAS weakness that is resistant to conventional treatment and severe enough that the patient would consider a colostomy, is a rare condition. The aetiology within this group is varied and our patients reflected this. All patients had poor internal sphincter function, although there was a range of causes.
Two patients had a normal anal resting pressure but persistent incontinence. One of these patients had a fragmented internal sphincter. A normal anal resting pressure associated with passive incontinence has been described previously.21,22 Passive leakage may occur as a result of segmental weakness or due to excess sphincter relaxation.
It has been shown that IAS defects are not amenable to simple surgical repair and weakness of the IAS is usually not improved after post-anal repair.6,7 Previous studies using injectable agents for the treatment of faecal incontinence have shown mixed results.11–,14 In a pilot study16 we showed that optimal results for the injection of Bioplastique were obtained using circumferential injections, at three separate sites, using a 2.5 inch needle tracked trans-sphincterically. This technique, combined with the use of 160 mg gentamicin and 500 mg metronidazole intravenously immediately prior to the procedure, and oral cephalexin (500 mg four times daily) and metronidazole (400 mg three times daily) for seven days post-procedure, has resulted in no complications. In a previous pilot study there were complications of either leakage or infection using a 1 inch needle to inject Bioplastique directly into the region of the lower IAS, through the anal mucosa, and using a single dose of 80 mg gentamicin intravenously and cephalexin 500 mg four times daily orally for only five days after the procedure.
There was a marked improvement in the SF-36 quality of life scores in both the social function and physical function subscales after injection with Bioplastique (p=0.02). The incontinence score also improved but not to such a dramatic extent (p=0.04). This may be due to a lack of sensitivity in the incontinence scoring system that has not accurately reflected the clinical improvement that was seen in patient symptoms. Continence scores are insensitive for assessing the amount and frequency of passive incontinence. In addition, the overall support and infrastructure, provided by a specialist unit, may contribute to improved quality of life. Generic tools such as the SF-36 and continence scores measure different parameters. The SF-36 is affected by many different factors, such that changes in continence are likely to have only a partial effect. This results in limited correlation between changes in the generic SF-36 and the disease specific incontinence score.
The underlying physiological changes in anal sphincter function that were responsible for the marked clinical improvement may or may not relate to the demonstrated changes in anal manometry. Circumferential injection of Bioplastique at three sites caused the resting anal pressure to rise by a median of 63% (p=0.02). Vascular filling of the anal cushions in the normal individual is thought to contribute up to 15–20% of the resting pressure,23 providing a compliant watertight seal at the anal margin. The bulking effect of the silicone injections may be enhancing the action of the naturally occurring anal cushions which provide closure in the gap inside the internal sphincter ring.24
While it was expected that successful injections might cause an increase in the resting pressure, a beneficial effect on the external sphincter function was not anticipated. Squeeze pressures rose by a median of 45% (p=0.1). Although not statistically significant, this may represent an improvement in the function of the external anal sphincter. It is more probable however that this increase was due to the physical bulking effect of the three injections.
The endoanal ultrasound scans confirmed the presence of the injected Bioplastique at the appropriate position within or around the IAS in the five of six patients who showed a benefit, with no evidence of local migration. Distant migration, although unlikely, was not assessed. The level of the Bioplastique was at the upper part of the anal canal extending up to and just beyond the puborectalis ring, marking the upper limit of the anal canal. In the one subject in whom there was no improvement, the Bioplastique had migrated out of the high pressure zone of the anal canal and was lying above the puborectalis ring. This has implications for future injections in that the optimum site seems to be at the IAS just above the dentate line, allowing pain free injections, but below the puborectalis ring so that the injection remains within the upper anal canal.
The continuing clinical and physiological benefit shown in these patients combined with the persistent findings on endoanal ultrasound suggest that the use of Bioplastique as a bulking agent will not be associated with problems of migration and absorption experienced with previous bulking agents.11 In addition, combining a trans-sphincteric injection technique with an aggressive antibiotic regimen avoided the previously experienced complication of infection. Animal studies have shown that the carrier gel, PVP, is excreted over a three day period, leaving the non-absorbable non-biodegradable silicone particles. The gel is then slowly replaced by a fibrin and protocollagen matrix that surrounds the silicone particles, which at six weeks becomes stabilised with collagen fibres.25,26 This forms the permanent bulking agent that augments the IAS.
In this study we have shown that outpatient injection of a silicone based biomaterial can provide a marked improvement in faecal incontinence due to a weak or disrupted IAS. Continence and quality of life seem to have improved in the medium term and there was a corresponding physiological improvement in sphincter function. Longer term outcome needs to be assessed.