Article Text

Abstract
Objective Interval colorectal cancers (interval CRCs), that is, cancers occurring after a negative screening test or examination, are an important indicator of the quality and effectiveness of CRC screening and surveillance. In order to compare incidence rates of interval CRCs across screening programmes, a standardised definition is required. Our goal was to develop an internationally applicable definition and taxonomy for reporting on interval CRCs.
Design Using a modified Delphi process to achieve consensus, the Expert Working Group on interval CRC of the Colorectal Cancer Screening Committee of the World Endoscopy Organization developed a nomenclature for defining and characterising interval CRCs.
Results We define an interval CRC as a “colorectal cancer diagnosed after a screening or surveillance exam in which no cancer is detected, and before the date of the next recommended exam”. Guidelines and principles for describing and reporting on interval CRCs are provided, and clinical scenarios to demonstrate the practical application of the nomenclature are presented.
Conclusions The Working Group on interval CRC of the World Endoscopy Organization endorses adoption of this standardised nomenclature. A standardised nomenclature will facilitate benchmarking and comparison of interval CRC rates across programmes and regions.
- COLORECTAL CANCER
- SCREENING
Statistics from Altmetric.com
Video abstract
Significance of this study
What is already known on this subject?
Interval colorectal cancer (interval CRC) rates are an important indicator of the quality and effectiveness of screening programmes.
Variability in definitions used for an interval CRC precludes accurate comparisons of rates across studies and programmes.
What are the new findings?
Using a modified Delphi process, the Expert Working Group on interval CRC of the Colorectal Cancer Screening Committee of the World Endoscopy Organization developed a standardised nomenclature for defining and reporting on interval CRCs.
How might it impact on clinical practice in the foreseeable future?
A standardised nomenclature will facilitate benchmarking and comparison of interval CRC rates across programmes and regions.
Introduction
As evidence accumulates demonstrating the effective-ness of colorectal cancer (CRC) screening1–7 and population screening is increasingly adopted as a public health initiative worldwide, interest in interval CRCs, or cancers occurring after a negative screening or surveillance exam, is growing. While no screening test will ever be perfect, the frequency of failures is a marker of the quality and effectiveness of a screening programme. Minimising the occurrence of interval CRCs is important for assuring the quality of a screening programme. Better measurement of interval CRCs will enable screening programmes to identify performance gaps that can be addressed to improve effectiveness.
Although observational studies indicate that colonoscopy and polypectomy is associated with a reduction in the incidence of8–10 and mortality from10–12 CRC, there is a large operator-dependent variability in the quality of examinations,13–16 which likely contributes to variable effectiveness of colonoscopy, especially in the proximal colon.17–19 Likewise, the sensitivity and specificity of faecal tests in detecting colorectal neoplasms vary.20 In order to compare the effectiveness of programmes and tests, a standard definition for quality measures such as interval CRCs is needed. For example, reports on interval CRC have included in their definition cancer diagnosed from <3 years, to <5 years, to <10 years to an unlimited time after index colonoscopy.21–24 Lack of consistency in the definition of interval CRC precludes meaningful comparisons across studies and programmes, and hinders progress towards understanding and addressing their causes.
The Expert Working Group on interval CRC of the Colorectal Cancer Screening Committee of the World Endoscopy Organization (WEO) reviewed the previously used definitions of interval CRCs with the goal of developing a nomenclature for defining interval CRCs to facilitate benchmarking and comparison of interval CRC rates across studies and programmes internationally. Our goal was to develop a definition that could be applied after screening or surveillance exams. Using a modified Delphi process to develop and achieve consensus, we offer a standardised nomenclature for interval CRCs and a practical guideline for determining and reporting on interval CRCs.
Methods
Membership of the Consensus Panel
Criteria for eligibility to the Consensus Panel were (1) demonstrated knowledge/expertise by previous or current research on interval CRCs, peer-reviewed publications in the field or participation in national or regional guideline development; (2) wide geographical representation (including Europe, North America, Australia); and (3) diversity of training expertise (including gastroenterology, pathology, epidemiology and public health). The Consensus Panel comprised eight members, who were identified by the WEO chairs through invitation.
Literature review
We conducted an electronic search on PubMed and Cochrane databases using the following keywords: Colorectal Neoplasms [Mesh]; colorectal cancer; colorectal cancer screening; interval colorectal cancer; post colonoscopy colorectal cancer; fecal immunochemical test; FIT; guaiac fecal occult blood test; gFOBT; FOBT; fecal occult blood test; stool test; Colonoscopy [Mesh]; colonoscopy; negative colonoscopy; Sigmoidoscopy [Mesh]; sigmoidoscopy; negative sigmoidoscopy. Searches were limited to English-language articles published in the preceding 10 years (from January 2004 to January 2014). Relevant studies included those in which identification of interval CRCs and estimation of rates were primary or secondary goals. We also reviewed original studies on the effectiveness of screening (with any test modality) in reducing the incidence of CRC. We obtained information on interval CRCs from national and regional CRC surveillance guidelines.25–31 To maximise the output of our search, we retrieved additional articles extracted from the reference list of the reviewed articles. We examined the effect of the definition used for an interval CRC, after screening or surveillance exams, on the estimated rates of these outcomes. Secondary goals were to identify salient features of interval CRCs (e.g., time to diagnosis, anatomic location, cancer stage at diagnosis and histology), as well as their putative aetiology (e.g., missed, incompletely resected polyps or biologic factors associated with a more rapid progression). We excluded studies in persons with hereditary CRC syndromes or inflammatory bowel disease.
Modified Delphi process
To develop and achieve consensus on a standardised nomenclature for interval CRCs, the Consensus Panel used a modified Delphi process.32 The Delphi process encompasses a stepwise approach, including (1) summarising the literature and rating the quality of evidence, (2) developing consensus statements and (3) achieving consensus through in-depth discussions and subsequent voting. After a systematic literature review by two of the authors (SS, CMClC), narrative summaries were circulated to the members of the Consensus Panel and frank discussion and debate were encouraged. During four meetings (Digestive Disease Week 2013, May 2013, Orlando, Florida, USA; World Congress of Gastroenterology 2013, September 2013, Shanghai; United European Gastroenterology Week 2013, September 2013, Berlin; and the Digestive Disease Week 2014, May 2014, Chicago, Illinois, USA) and nine teleconferences, the Consensus Panel analysed and rated the evidence. An analytic, case-based approach was used to maximise participation and provide a framework for developing the nomenclature. Subsequently, two of the authors (SS, RES) drafted a list of statements and circulated it electronically. In total, three sets of consensus statements were defined: the first set (statements 1–10) aimed to ensure consistency regarding knowledge and view about the current literature, in particular the definitions employed for interval CRCs, study methodology, incidence rates and the potential etiologic factors. For each statement, a summary of the current evidence, rating according to the GRADE methodology33 and discussion of the areas of uncertainty and controversy were included. A second set (statements 11–16) aimed to define criteria for standardising the nomenclature. The third set (validation set) tested the level of agreement between the Consensus Panel members on the nomenclature in a series of 12 clinical examples. Each member was asked to consider the evidence to support or refute the statements and to rate it on a Likert scale ranging from 1 to 5: 1, accept completely; 2, accept with minor reservation; 3, accept with major reservation; 4, reject with reservation; and 5, reject completely. The first vote was conducted electronically and simultaneously for the entire Consensus Panel, without explanation or justification of each statement. Feedback was then obtained from all members. The results and the comments were subsequently evaluated by two authors (SS, RES). Consensus was considered to be achieved when >80% of the voting members indicated ‘accept completely’ or ‘accept with reservation’, and refuted when >80% of the voting members indicated ‘reject completely’ or ‘reject with reservation’. Finally, a teleconference was organised to review the evidence with respect to each statement that reached consensus and discuss again those statements that did not reach consensus on the first voting. A second vote was held following the teleconference. All members of the consensus process were given ample opportunity for input into the final wording of the consensus document. The final document was peer reviewed by the WEO Chairs and approved in accordance with the WEO Publication Policy.
Results
Literature review on interval CRCs
The membership of the Consensus Panel agreed that the nomenclature currently employed for interval CRCs varies considerably, hindering comparison across studies. Online supplementary table S1 presents the consensus statements and the corresponding levels of evidence and agreement between the panel members. In this section, we detail the definitions used and their effect on interval CRC rates.
Interval CRC after a colonoscopy
In 1997, Haseman et al34 described a series of 47 cases of CRC diagnosed within 3 years after a colonoscopy; 27 of them were considered missed cancers, while 20 cases were likely the result of an incomplete colonoscopy. Performance of colonoscopy by a non-gastroenterologist was associated with greater odds for an interval cancer (OR 5.46, 95% CI 2.94 to 9.77). Since then, gastroenterology specialists around the world have extensively addressed the magnitude of this problem and its putative explanations. In tables 1 and 2, key studies estimating rates of interval CRC after colonoscopy in different populations are summarised.
Overview of studies on interval CRCs after colonoscopy in asymptomatic populations, showing that variation in the definitions used for an interval CRC affects the estimated rates
Overview of studies on interval CRCs after colonoscopy in a mix of symptomatic and asymptomatic populations, showing that variation in the definitions used for an interval CRC influences the estimated rates
The members of the Consensus Panel acknowledged striking differences in the definition of an interval CRC: in particular, the minimum time elapsed from the baseline colonoscopy to diagnosis of an interval cancer ranged from 6 to 60 months in the majority of studies,11 ,17 ,18 ,35–41 but exceeded 10 years in others.24 ,42 For example, in a study by Bressler et al17 in Ontario, Canada, the overall proportion of interval CRCs after colonoscopy was 3.4% when including cancers diagnosed within a 3-year interval of a negative exam versus 4.6% when extending the interval to 5 years. Epidemiological models indicate the ‘mean sojourn time’ for cancer (e.g., the estimated interval between the asymptomatic (screening) and the symptomatic phase) may be longer than previously assumed, ranging from 4.5 to 5.8 years.43 A time cut-off of 3 years may underestimate the proportion of interval CRCs. A 3-year cut-off will likely capture interval CRCs after missed lesions, but may miss those due to slower growing precursor lesions.39 ,44 ,45
As detailed in tables 1 and 2, the reported proportions of interval CRC vary greatly, ranging from 0.8% of colonoscopic examinations46 to up to 9% of all diagnosed CRCs.19 However, the number of interval CRCs/number of colonoscopic examinations performed is not comparable to the number of interval CRCs/total number of CRCs. Studies from Ontario and Manitoba, employing claims-based administrative data, found that proportions of interval CRC within 3 years after prior colonoscopy ranged from 3.4% to 9.0%.17 ,18 ,19 ,47 These studies could not include details on the quality of the baseline colonoscopy, such as cecal intubation rate or adenoma detection rate (ADR). In a Polish colonoscopy-based screening programme, Kaminski et al48 found a rate of 42 interval CRCs among 45 026 subjects during 188 788 patient-years of follow-up. Endoscopists’ ADR was significantly associated with the risk of interval CRC (HR 12.5, 95% CI 1.5 to 103.4 for ADR of 15.0% to 19.9% versus ≥20%, p=0.02). Endoscopists who performed a lower number of colonoscopies were excluded, which may underestimate the total number of interval CRCs in the population. In a recent study, using data from an integrated healthcare delivery system in the USA, the ADR was inversely associated with the risks of interval CRC, advanced-stage interval CRC and fatal interval CRC.49
The Consensus Panel also agreed that there was a wide variation in the methodological evaluation of interval CRCs across studies, including retrospective,17 ,23 ,36 ,37 ,48 ,50–52 prospec-tive,21 ,22 ,38 ,40 ,44 ,53 ,54 programmatic versus opportunistic screening, use of claims-based administrative data18 ,22 ,36 ,45 ,47 versus clinical records,23 ,24 ,37 ,39 ,42 as well as differences in study populations (age group included and proportion of men, inclusion of average- versus higher-risk groups; and screening versus surveillance settings). Methodological variation likely influenced the reported proportions of interval CRCs. For example, the study by Kaminski et al48 included persons aged 40–66 years, 35.7% of whom were men. The study by Singh et al18 included persons aged 50–80 years, 57.5% of whom were men. As CRC is associated with older age and male sex, inclusion of a significant proportion of younger women would reduce interval CRC rates. Rigorous documentation of the clinical characteristics of the included populations is important for comparisons of interval CRC rates across studies.
Only a few investigators have examined predictors of interval CRCs, such as endoscopists’ specialty,17 ,18 ,48 hospital versus non-hospital setting17 or a family history of CRC.9 ,54 Few applied a structured algorithm to estimate the underlying aetiology.38 ,44 In a study of 2079 subjects enrolled in a polyp prevention trial, Pabby et al44 sought to estimate the proportion of interval CRCs due to procedural factors versus aggressive tumour biology. Using an algorithm, the authors estimated that 13 persons in 5810 person-years of follow-up developed interval CRCs, with 54% (n=7) being ‘avoidable’ (three missed and four incompletely resected polyps). Others found that procedural factors (e.g., incomplete colonoscopy, suboptimal bowel preparation, missed or incompletely resected lesions) could have made an even greater contribution to the occurrence of interval CRC (71–86%).38 ,39 ,45 Missed lesions, which may explain over 50% of interval CRCs,38 ,39 ,45 are difficult to distinguish from newly developed CRCs since classification and distinction rely on assumptions regarding the ‘mean sojourn time’44 of adenomas evolving into cancer. Describing a cancer as missed is impossible to prove since it is impossible to prove a precursor lesion was present when it was not initially detected. Studies examining the molecular characteristics of interval CRCs, such as those demonstrating higher rates of microsatellite instability and CpG island methylator phenotype (CIMP)-high status,10 ,55 ,56 may help to improve classification of interval CRCs by better defining the biological characteristics of tumours more likely to rapidly progress.
Few studies contain details about the process for interval CRC identification and the method used for estimating rates. For example, in the study by Farrar et al,37 the proportion of interval CRC was calculated as follows: proportion of interval CRC=(number of persons with CRC who had a previous colonoscopy 6–60 months prior to CRC diagnosis)/(total number of persons with CRC identified), resulting in a proportion of 5.4%. Other authors17 ,18 ,36 used a different approach: proportion of interval CRC=(number of persons with CRC who had a previous colonoscopy 6–36 months prior to CRC diagnosis)/(total number of persons with CRC identified), resulting in proportions of 3.4%,17 5.4%18 and 7.2%, respectively.36 The time cut-off in including a cancer as an interval CRC affects the overall proportion. If the cut-off had been 3 months instead of 6 months, or if diagnoses up to 60 months were included, the final proportions would have been altered.
Interval CRCs after flexible sigmoidoscopy
There is a wide variation in the definition of an interval CRC after a FS, as detailed in table 3. Although four high-quality randomised controlled trials of FS are available,4 ,5 ,57 ,58 definitions of interval CRC after FS lack uniformity and the estimated rates are again not comparable.
Overview of studies on interval CRCs after flexible sigmoidoscopy (FS)
FS-based screening, with subsequent colonoscopy in case of a positive examination, is associated with incidence rates of interval CRCs ranging from 0.3 to 0.9 per 1000 FS exams, corresponding to higher and lower rates of adenoma detection, respectively.59 Others have reported crude numbers of interval CRCs.5 ,57 ,58
Analyses of the aetiology of interval CRCs are few.58 ,59 In the Prostate, Lung, Colorectal, and Ovarian (PLCO) FS trial, the authors classified CRCs into three categories: (1) screen-detected (within 12 months of a positive finding on FS); (2) not detectable (early-stage CRCs identified >30 months or advanced CRCs identified >48 months after a negative screening FS); or (3) prevalent, not-detected (early-stage CRCs identified <30 months and advanced CRCs identified <48 months after a negative screening FS). Over 11 years of follow-up, the proportion of screen-detected, not detectable and prevalent not-detected CRC was 24.9%, 48.1% and 27.0%, respectively.58 Among prevalent not-detected lesions, 35.6% were attributed to patient non-compliance, 43.9% to the limitations of FS relative to colonoscopy and 20.5% (n=54) to missed lesions.
Interval CRC after a faecal test
Unlike interval CRCs after endoscopic examination, there is greater uniformity in the definition of an interval CRC after faecal testing (table 4). The most common definition used was “CRC detected after a negative faecal occult blood screening test and before the next invitation is due”. However, the studies used various tests (guaiac faecal occult blood test (gFOBT) versus faecal immunochemical test (FIT)) at different frequency (yearly or biennially) and at different cut-off concentrations for a positive faecal occult blood test in diverse populations. Lack of standardisation in the reporting units for FIT (e.g., micrograms of haemoglobin per gram of faeces) may have also contributed to differing results.60 Only a few studies have examined interval CRCs after multiple rounds of faecal occult blood testing.61–63
Overview of studies on interval CRCs after faecal testing
In a study of 3616 screening participants,62 the authors found that 10 of a total of 39 CRCs (25.6%) identified after two rounds of faecal testing were interval CRCs: nine following a negative FIT or gFOBT and one following a negative colonoscopy. In an evaluation of the National Health Service Bowel Cancer Screening Programme in England, in 534 411 participants, 192 of 1336 CRCs (14.4%) identified were interval CRCs, all of them following a negative gFOBT.64
Proposed nomenclature for interval CRCs
Following a critical appraisal of the literature, the Consensus Panel defined key principles for creating a standardised nomenclature. A substantial agreement was achieved between the panel members with regard to the definition and classification of interval CRCs, as detailed in online supplementary table S1.
Definition of an interval CRC
The Expert Working Group on interval cancers of the Colorectal Cancer Screening Committee, WEO defines an interval CRC as a “colorectal cancer diagnosed after a colorectal screening examination or test in which no cancer is detected, and before the date of the next recommended exam”. This definition is derived from the International Agency for Research on Cancer (IARC) definition of interval cervical cancer, which is defined as an “invasive cancer diagnosed in an attender after a negative screening; and before the next invitation to screening was due” (IARC Handbooks of Cancer Prevention; Cervix Cancer Screening).65
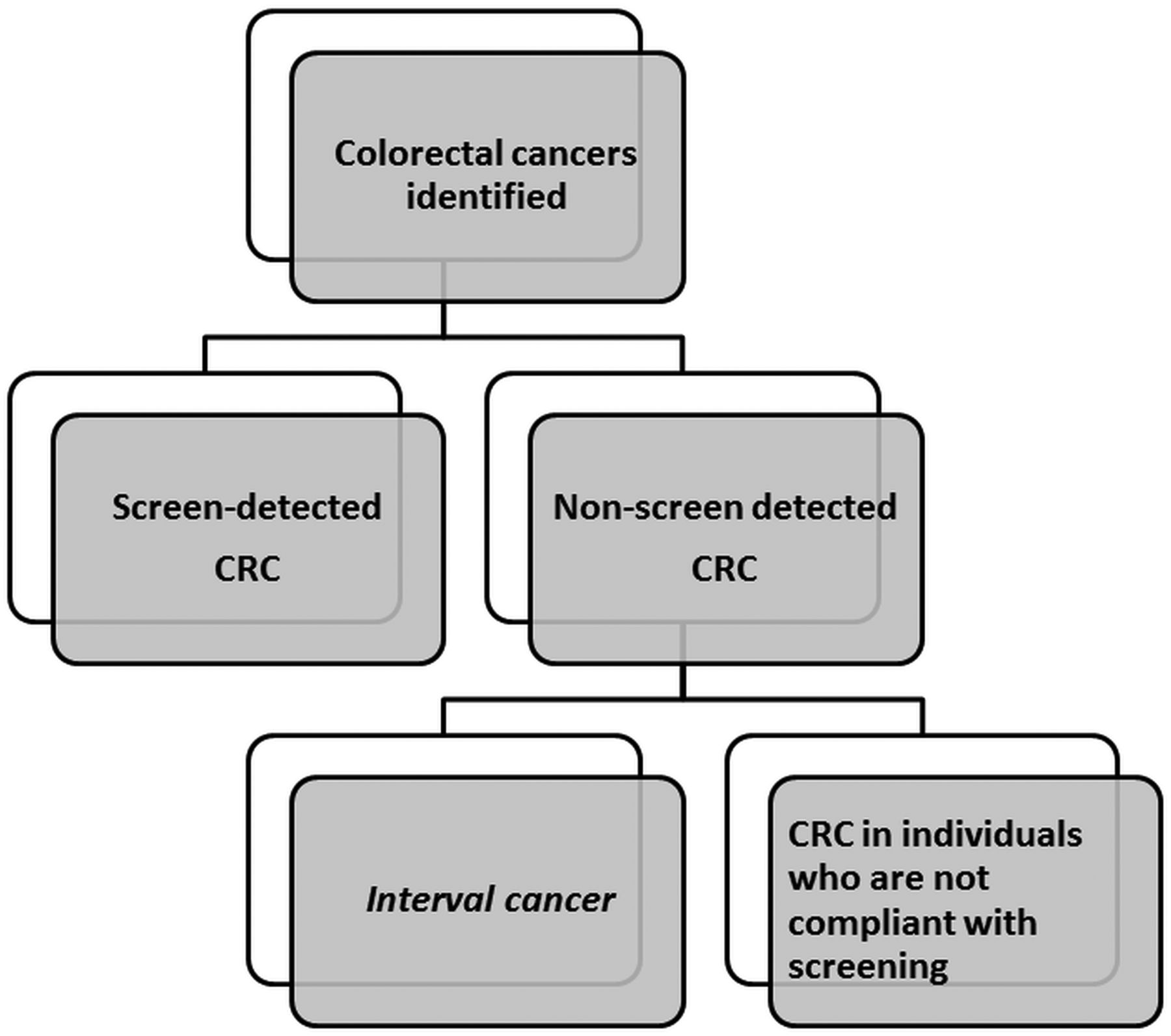
In the framework of an organised screening programme, systematic reporting of (1) screen-detected CRCs, defined as cancers diagnosed within the screening programme, and at a defined period after a positive screening test/examination; and (2) non-screen-detected CRCs, which can include interval CRCs, as defined above, and cancers in individuals who are not compliant with screening, is recommended (figure 1).66 Interval CRCs, by definition, do not apply to those who are not compliant with screening since there cannot be an interval CRC if the individual did not undergo initial testing. The proposed nomenclature applies to screening (with any modality) and colonoscopy surveillance. A CRC diagnosed during colonoscopy surveillance but before the date of the next recommended exam will qualify as interval CRC. When the screening interval is not provided, standard intervals should be employed (such as 2 years for FIT/gFOBT, 5 years for FS and 10 years for colonoscopy). In the circumstance of a once-only screening programme, since no repeat exam is recommended, there is no opportunity for an interval cancer.

{kind=link}
Proposed nomenclature for classification of colorectal cancers. The nomenclature applies to screening (with any modality) and colonoscopy surveillance. CRC, colorectal cancer.
In order to apply the definition of an interval CRC in an organised, reproducible manner, the Consensus Panel recommends the following principles regarding classification:
Designation of the test/examination that preceded the diagnosis of cancer
Interval CRC rates should be reported with the designation of the test that preceded the subsequent diagnosis of cancer.
For example, within a FIT screening programme, a CRC after a negative FIT screening test but before the next FIT is due would be designated as a ‘FIT interval CRC’. Likewise, within a CS screening programme, a CRC after a negative screening CS but before the next recommended procedure would be designated as a ‘CS interval CRC’.
Designation of the test/examination to which an interval CRC should be attributed
The screening test to which an interval CRC is attributed should refer to the most recent, most comprehensive examination performed prior to cancer diagnosis. For example, a cancer after a positive FIT screening test and a subsequent negative colonoscopy (but before the interval for the next FIT is due) would be considered a CS interval CRC and not a FIT interval CRC.
Designation of the context in which the interval cancer arose
Screen-detected and non-screen-detected cancers can be reported in the context of the programme, which led to diagnosis, for example, FIT biennial screening, primary CS or FS screening. In the case from principle 2, though a CS interval cancer, the context was that of a programme of FIT testing, so this cancer can be designated as a “CS interval cancer (within a FIT screening programme).” In the case of a CS interval CRC, the context can be further described, such as an interval CRC within a screening programme or following opportunistic screening.
Numeric calculation and reporting of interval CRC rates
Ideally, screen-detected and non-screen-detected cancers should be reported as numbers per 100 000 person-years of observation.44 This measure reflects the observed person time at risk and accounts for loss to follow-up. In contrast, reporting rates per 1000 persons invited to participate (intention-to-screen) may preclude accurate comparisons because of variability in participation. The European guideline for quality assurance in CRC screening and diagnosis67 recently recommended a comprehensive approach to interval CRC rates calculation, adjusting for the CRC incidence in the background population, as well as age-specific and sex-specific variations.
Minimum data set
The Consensus Panel recommends inclusion of the following data for the documentation of interval CRCs: demographic features (age, sex) of the affected subject and the overall population; the indication for the procedure (e.g., screening, surveillance exam or symptoms); the initial test employed (e.g., gFOBT, FIT, FS, CS); the context in which the test was performed (e.g., organised screening programme versus opportunistic screening); the recommended surveillance interval (where applicable); the upper age limit for screening (where applicable); the time elapsed from the screening test to CRC diagnosis; and the location, the histopathology and the cancer stage at diagnosis of the CRC. In the case of FIT screening, the test characteristics should be included, in particular the type of test (including type of buffer) and the analytic measurement device. If referring to a quantitative FIT device, the cut-off concentration for a positive test in microgram haemoglobin/gram faeces should be included.
Practical application of the nomenclature
Table 5 shows examples of case scenarios with the attached interval cancer classification to demonstrate the practical application of the nomenclature. Substantial agreement was obtained among the membership of the Consensus Panel when evaluating these cases. Online supplementary table S2 presents samples of minimum data sets corresponding to the previous clinical case scenarios.
Case examples illustrating the practical applicability of the nomenclature
Notable features of the proposed nomenclature should be acknowledged. First, the IARC definition of interval cancers has been extended to CRC arising during colonoscopy surveillance. To ensure consistency with the IARC nomenclature, the Consensus Panel restricted the definition to ‘invasive cancer’ and did not include advanced or non-advanced adenoma. Because there is international variation in the recommended timing of repeat screening and surveillance exams, the nomenclature preserved the term ‘recommended exam’ in the definition. This means that interval cancer rates may vary by local or regional practice due to variation in when exams should be repeated. Thus, clear documentation of the recommended dates for a repeat exam must be included. The proposed nomenclature provides general principles for determining and reporting interval CRCs. Complex situations can arise, which will prove challenging (e.g., multiple FIT screening episodes, single FS screening followed by FIT biennially, etc). Finally, identification of interval CRCs requires resources to support organised, systematic reporting. Better insight into the underlying biological processes driving interval CRC formation and a more extensive understanding of the endoscopic performance characteristics associated with interval CRC will facilitate reduction of their occurrence. Future work will aim to develop criteria for adjudicating the causes of interval CRCs during screening and surveillance (e.g., missed, incompletely resected or rapidly progressive neoplasms).
In conclusion, principles for defining and categorising interval CRCs after screening or colonoscopy surveillance exams and a proposed nomenclature are presented. Clinical scenarios to demonstrate the practical application of the nomenclature are provided. The Expert Working Group encourages adoption of this standardised nomenclature. A standardised nomenclature will facilitate benchmarking and comparison of interval CRC rates across programmes and regions internationally.
Acknowledgments
The comments and suggestions contributed by Stephen P. Halloran, UK; Helen Seaman, UK; Sidney J. Winawer, USA; Carlo Senore, Italy; Samir Gupta, USA; and Ernst J. Kuipers, NL are gratefully acknowledged.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
Contributors SS and RES: study concept and design; literature review; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. CMClC: literature review; analysis and interpretation of data; technical support. GAM, LR, ED, MDR, RV and GPY: study concept and design; analysis and interpretation of data; critical revision of the manuscript for important intellectual content. All authors approved the draft manuscript to be published.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.