Article Text

Abstract
The treatment of pectoralis major tendon ruptures has been the subject of much debate. The classical history of the injury is forced abduction and external rotation. The cases of two patients (an amateur rugby union player and a recreational snowboarder) are reported. The diagnosis was made by clinical examination in both patients, and both were operated on more than two weeks after injury. After surgery and a graduated rehabilitation programme, both men were able to return to their sporting activities. These two cases highlight the advantage of operative management in this uncommon condition.
- pectoralis major tendon
- rupture
- surgery
Statistics from Altmetric.com
The pectoralis major is an extremely powerful adductor, internal rotator, and flexor of the humerus. Its importance in contact sports stems from its action as a dynamic stabiliser of the shoulder.1 It forms the anterior wall and fold of the axilla, extending across the front of the axilla to insert on to the proximal humerus. It originates in the medial clavicle, the sternum, the aponeurosis of the external oblique muscle, and the cartilages of the first six ribs. It has an unusual humeral insertion in that the clavicular and upper sternal fibres attach distally on the humerus, while the lower sternal and abdominal fibres cross above the former and insert uppermost on the shaft of the humerus (fig 1).

Normal anatomy of the pectoralis major muscle. There is a distinct orientation of the clavicular head (C) at the superior margin of the chest, as well as a sternal head (S) more inferiorly. Reproduced, with permission, from Connell et al.7
This condition was first described by Patissier in 1822,2 followed by Letenneur in 1861.3 To date, only about 150 cases have been reported in the English language, with the bulk being in the last 25 years.
Rupture of this muscle is an uncommon sports injury that has become considerably more prevalent in the last 30 years as the numbers of both professional and recreational athletes increase. Common activities associated with this injury include weight lifting (especially bench pressing), wrestling, American football, and rugby football.
Injury to the pectoralis major muscle is usually caused by a sudden forceful overload of the maximally contracted muscle. This is different from the attritional ruptures associated with the rotator cuff or biceps tendon.4 The patient usually gives a history suggesting a powerful contraction of the muscle or a direct blow applied to the shoulder region, with his/her arm in the adducted position.
Patients with pectoralis major tendon ruptures classically present with a history of sudden severe pain in the arm and shoulder at the time of injury, with or without a “snap”, painful limitation of motion, localised swelling and ecchymosis, and weakness.5
Physical examination shows a thin anterior axillary fold or even a sulcus at the deltopectoral groove. Tensioning of the pectoralis muscle creates bulging at its origins on the chest. Muscle testing shows weakness in adduction and internal rotation of the arm. Because of the rarity of this condition, the symptoms and signs may be missed on initial presentation. Sequential clinical examination is helpful in this regard.
CASE 1
A 25 year old amateur rugby union footballer was wrestling for the ball in a loose ruck situation when he was impacted from the side by another player. He felt sudden pain in the right pectoral region and had to stop playing. On the following day, the deltopectoral area was swollen, tender, and very bruised. Movement about the shoulder was reduced and associated with pain, especially during adduction and forward flexion of the humerus.
After this episode, the patient reported a definite decrease in the power of flexion and adduction. With the subsidence of the pectoral area swelling, a definite step was palpable in the anterior axillary fold. He was initially treated non-operatively, but presented to the senior author (BJH) at three months, complete with an internet literature search, requesting surgical intervention. He was unwilling to accept the permanent weakness.
CASE 2
A 24 year old male was snowboarding when his arm became jammed against the ground causing forced extension and external rotation of the humerus. He felt pain in the right pectoral region. Over the ensuing days, the area became very swollen and bruised, with a step palpable in the anterior axillary fold. During the following months, he reported that his arm tired very easily, and that he had difficulty rising from chairs. On examination, the pectoralis major muscle bunched up when stressed. He presented nine months after his injury.
IMAGING AND STAGING
In both cases, plain radiographs showed no bony abnormality. The absence of the pectoral shadow has been postulated as a confirmation of clinical diagnoses.
The use of ultrasound has been advocated to visualise tears, by virtue of uneven echogenicity and muscle thinning compared with the opposite side. Computed tomography scanning can also be used to show disruption of the muscle tendon. However, magnetic resonance imaging (MRI) has been cited as the most useful imaging modality. Ohashi et al6 found that axial T2 weighted images were most useful for acute and subacute injuries, whereas axial T1 weighted images were most useful for delineating chronic injuries. MRI can also visualise haematoma in the muscle belly, suggestive of proximal tears.
Connell et al7 imaged 15 patients with pectoralis major muscle tears using MRI. They found that their results correlated well with surgical findings and concluded that MRI allows accurate evaluation of injuries of the pectoralis major muscle and enables identification of patients who would benefit from surgical repair.
Attempts have also been made to grade these injuries, both clinically and with imaging, with perhaps the best being suggested by Tietjen.8 His classification is: 1, contusion or sprain; 2, partial tear; 3, complete tear; 3A, muscle origin; 3B, muscle belly; 3C, musculotendinous junction; 3D, muscle tendon itself.
Despite the advances in imaging and classification, the diagnosis of this condition is still essentially a clinical one. When treating these patients, it is worth remembering the findings of Marmor et al.9 Using muscle testing, they showed that the pectoralis major muscle is not necessary for normal shoulder function, but is important for carrying out strenuous activities. Thus, patients who wish to return to active athletic pursuits (the vast majority) are likely to benefit from surgery, whereas the more sedentary and elderly may be treated conservatively.
SURGERY
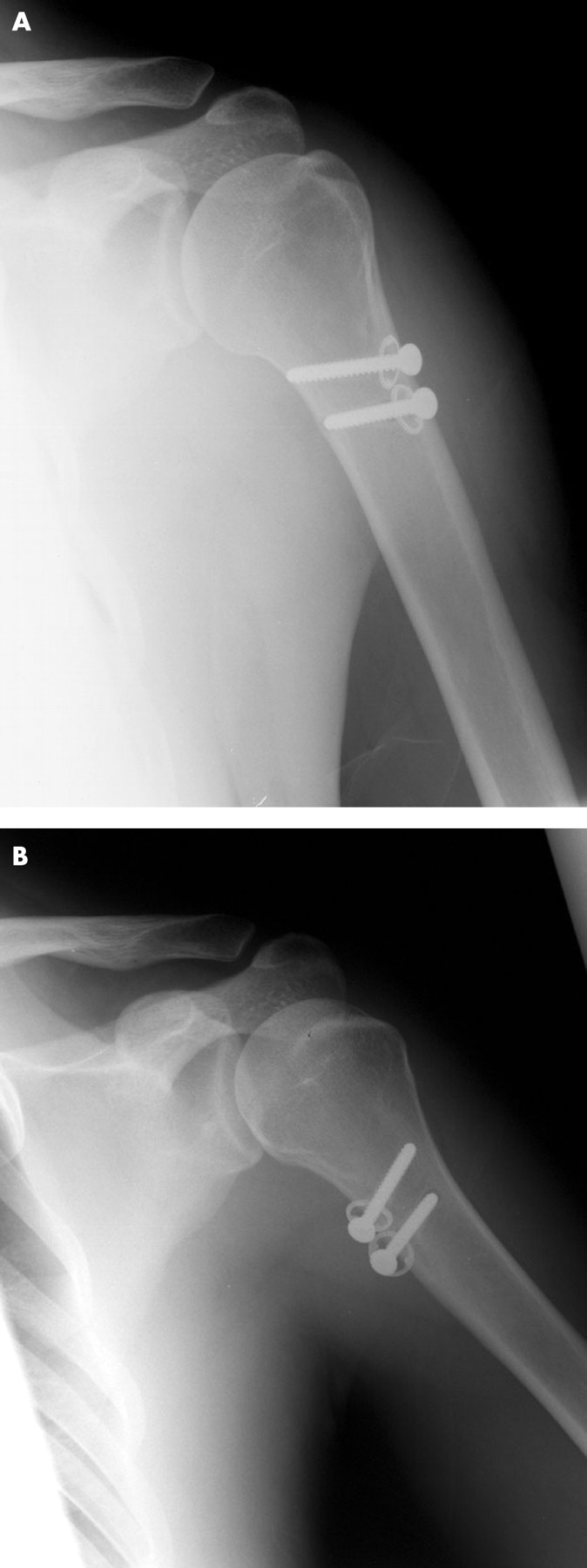
The two patients in this series had similar surgical procedures. They were draped and prepared in the beach chair position. Through a deltopectoral incision, the free ends of the tendon were identified. The adhesions present were divided. The lateral lip of the bicipital groove was petalled using an osteotome. The ruptured tendon was then approximated to the roughened surface and fixed with two 4.5 mm cancellous screws with spiked plastic washers (fig 2).
{kind=link}
{kind=link}
Radiographs of surgical repair of ruptured pectoralis major muscle. Case 2.
After surgery, the arm was rested in a broad arm sling for the first six weeks, followed by a graduated rehabilitation programme, culminating in exercises against resistance. This programme is in keeping with other reported series.
The first patient reported that he was fully fit and able to resume his sporting career (rugby football) eight months after surgery. The second had subjectively regained full strength and function nine months after surgery.
A review of the literature shows that methods of operative management are essentially all variations on the same theme. Miller et al10 cite the use of bone anchors for fixation, while suture fixation also appears to be widely used. Burring a trough lateral to the biceps tendon and passing the suture through tendon and bone best achieve this. Schepsis et al11 report on the use of modified horizontal and vertical Kessler sutures to achieve their fixation.
ISOKINETIC TESTING
At 60 and 15 months after surgery respectively, patients 1 and 2 underwent isokinetic testing using the Biodex system.
The first patient showed right shoulder slow twitch fibres that compared very favourably with the left in terms of strength (peak torque). The right fibres were 3.8% stronger than the left, indicating right sided dominance. Total work values were equal between the two sides. At fast test speeds, the right flexors were considerably stronger than the left. The right was currently 25% stronger than the left, indicating considerable right sided dominance. Total work values on the right also indicated significant right sided dominance, indicating no strength deficit of this muscle group. The antagonistic muscle group and extensors also compared very favourably on the right at both slow and fast test speeds, indicating no significant strength deficit.
Take home message
Ruptures of the pectoralis major tendon cause both cosmetic and functional problems. Surgical repair, either early or late, is not difficult, and can restore normal cosmesis and full function.
Similarly, the second patient showed only a very mild strength variance of 3.7% between the affected and unaffected shoulders at the slow speed. The total work values also compared favourably, with a 2.5% variance. At the fast speed, there was only a 7% variance in terms of peak torque, with the fast speed variance being only 1.6%. The antagonist muscle group, the shoulder extensors, also compared very favourably, with variances of 1.2% and −8.3% at the slow and fast speeds respectively.
DISCUSSION
Pectoralis major tendon rupture is still an unusual injury, albeit one with an increasing incidence, as seen by the fact that most of the literature on the subject has been published in the last 25 years. This increase may be attributed to the increase in sporting pursuits, especially higher velocity sports, and the increase in strength and fitness of participants. The use of anabolic steroids has also been mentioned as being a contributory factor.8
The diagnosis of this condition is primarily clinical. Management may be surgical and non-surgical. In relation to resuming previous activity, even at recreational level as with our two patients, surgical repair, how ever it is achieved, is indicated. In many cases, patients are unwilling to accept weakness and limitation of movement, and surgery is therefore indicated.
It would appear that the timing of surgery in the repair of ruptured pectoralis major tendons is not critical, as can be seen from these two cases.
Acknowledgments
We thank Dr Marie-Elaine Grant, PhD, Chartered Physiotherapist for her assistance in the Biodex isokinetic testing of the two patients. We also acknowledge with thanks David Connell MD, and RSNA for allowing the reproduction of fig 1.7