Article Text

Abstract
Context The effects of fish oil on cardiac function, ventricular remodelling and functional capacity in patients with chronic heart failure (CHF) remain controversial.
Objective The aim of this meta-analysis was to evaluate effects of fish oil on cardiac function and related parameters in CHF patients.
Data Sources Medline, Embase, the Cochrane Library and references cited in related reviews and studies.
Study Selection Randomised controlled trials of fish oil supplementation on cardiac function in patients with CHF were identified.
Data Extraction Two investigators read all papers and extracted all relevant information. A fixed effect or, in the presence of heterogeneity, a random effect model, was used to estimate the combined effects.
Results 7 trials with 825 participants were included. Meta-analysis results showed that left ventricular ejection fraction was significantly increased (weighted mean difference (WMD) = 2.25%, 95% CI 0.66 to 3.83, p = 0.005) and left ventricular end-systolic volume was significantly decreased (WMD = 7.85 ml, 95% CI −15.57 to −0.12, p = 0.05) in the fish oil group compared with the placebo group, although left ventricular end-diastolic volume was not significantly affected. Meta-regression and subgroup analysis indicated that the improvement in left ventricular systolic function was more remarkable in patients with nonischaemic heart failure. Fish oil supplementation also improved the New York Heart Association functional classification and peak oxygen consumption in patients with non-ischaemic heart failure.
Conclusions Improvement in cardiac function, remodelling and functional capacity may be important mechanisms underlying the potential therapeutic role of fish oil for patients with CHF. These effects might be more remarkable in patients with non-ischaemic heart failure.
Statistics from Altmetric.com
Introduction
Chronic heart failure (CHF) is a complex clinical syndrome characterised by insufficient status of cardiac function, which can be caused by various structural or functional cardiovascular disorders.1 Despite impressive advances in medical management and device therapy in recent decades, CHF remains one of the leading causes of cardiovascular morbidity and mortality worldwide.2 ,3 Thus there is an urgent need for the development of novel treatment strategies for CHF despite the standard pharmacological therapies that have been recommended by current medical guidelines.4 ,5
Numerous clinical trials have shown supplementation with fish oil, which mainly consists of two categories of marine omega 3 polyunsaturated fatty acids—eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA)—may lower the risk of major cardiovascular events, such as myocardial infarction, sudden cardiac death (SCD), coronary artery disease and perhaps atrial fibrillation.6 ,7 Growing evidence from experimental and epidemiological studies suggested that fish oil intake could be beneficial for patients with CHF.8 ,9 Previous studies also indicated that fish oil could improve cardiac function and functional capacity in CHF patients; however, clinical trials have shown inconsistent results.10–16 Therefore, we performed a meta-analysis to systematically evaluate the effects of fish oil on cardiac function, remodelling and functional capacity in CHF.
Methods
The study complied with the recently reported Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.17
Search strategy
We performed a literature search in Pubmed, Embase and the Cochrane Library for relevant records up to November 2011, using the term ‘omega-3 fatty acids’, ‘fish oil’, ‘fish-oil’, ‘marine oil’, ‘eicosapentaenoic acid’, ‘EPA’, ‘docosahexaenoic acid’, ‘DHA’, ‘dietary therapy’ paired with the following: ‘heart failure’, ‘cardiac failure’, ‘cardiac dysfunction’, ‘ventricular dysfunction’, ‘ventricular insufficiency’ and ‘cardiomyopathy’. The search was limited to studies in humans. We also analysed reference lists of original and review articles using a manual approach.
Study selection
Studies were selected for analysis if they met the following criteria: (1) published as full length articles in any language; (2) reported as a prospective, randomised and placebo controlled trial with either a parallel or crossover design; (3) analysed adult patients (>18 years) with established CHF (regardless of the aetiology and severity of the disease) who were assigned to oral fish oil supplementation or placebo for at least 1 month, in addition to concurrent therapy; (4) reported data on at least one of the following outcomes: left ventricular ejection fraction (LVEF), left ventricular end-systolic volume (LVESV), left ventricular end-diastolic volume (LVEDV), New York Heart Association (NYHA) functional class and peak oxygen consumption (peak VO2) in the exercise test.
Data extraction and quality assessment
Two authors (WX and WW) independently performed the literature search, data extraction and quality assessment according to the inclusion criteria. Discrepancies were resolved by consensus. Extracted data included study design characteristics, patient characteristics (number, age, sex, baseline cardiac function and concurrent medications), intervention strategies (total dose of fish oil, ratio of EPA to DHA and composition of the placebo), follow-up duration and means (SDs) for changes in the aforementioned outcomes. For studies presenting results at more than one time point from the same groups of participants, we selected a single time point at which data from the maximum number of subjects were available to avoid a unit of analysis error, as indicated in the instructions in Cochrane's handbook.18 For studies with multiple intervention groups (eg, with different doses of fish oil), we split the shared control group into two or more groups with a smaller sample size to overcome a unit of analysis error, and included these two or more comparisons into the meta-analysis according to the instruction in Cochrane's handbook.18
The quality of the studies was judged by quality of randomisation, generation of random numbers, concealment of treatment allocation, blinding and reporting of withdrawals. Trials scored 1 point for each area addressed, with a possible score of between 0 and 5, where 5 represented the highest level of quality.19
Statistic analysis
All endpoints were estimated based on the change from baseline to follow-up, and pooled effects were presented as weighted mean difference (WMD) with 95% CI. Inter-study heterogeneity was formally tested using Cochrane's Q test, and significant heterogeneity was considered to exist if the p value was <0.10. The I2 statistic, which describes the percentage of total variation across studies that is due to heterogeneity rather than chance,20 was also examined, and a value of I2 >50% indicated significant heterogeneity. If Cochrane's Q test showed significant heterogeneity, a fixed effect model was used to calculate WMD and its 95% CI. By contrast, a random effect model was applied.21 Meta-regression and predefined subgroup analysis were performed to explore the possible source of heterogeneity. Median values of continuous variables were used as cut-off values for grouping studies. A sensitivity analysis was conducted to determine the stability of the pooled results. Furthermore, potential publication bias was assessed with the Egger regression asymmetry test22 and funnel plots; p values were two tailed and statistical significance was set at 0.05. Meta-analysis and statistical analysis were performed with Stata software (V.12.0; Stata Corporation) and RevMan software (V.5.1; Cochrane Collaboration, Oxford, UK).
Results
Search results
A total of 1250 articles were identified, and 1210 were excluded because they did not describe randomisation or controlling, or because the objectives of these studies were irrelevant to the present meta-analysis. Of the 40 potentially relevant articles screened, seven10–16 met the selection criteria (figure 1). Thirty-three articles were excluded because the participants in 25 trials did not have CHF; seven trials did not report any data of related outcomes and one trial included children.

Flow diagram of the study selection procedure.
Study characteristics
Overall, eight study arms from seven studies10–16 were included in the meta-analysis, which comprised a total of 825 patients with CHF, 433 in the fish oil group and 392 in the placebo group. The characteristics of the studies are presented in table 1. All studies were of parallel design. Six studies declared that the participants were clinically and haemodynamically stable CHF patients who received optimal medical therapy based on modern CHF treatment strategies, including diuretics and neurohormonal inhibitors, and the medication treatment was maintained during the follow-up interval,11–16 while the other study did not report the use of β blockers in the included patients.10 Mean age of the participants varied from 57 to 73 years. The aetiology of CHF was exclusively ischaemic in two studies,10 ,11 non-ischaemic in three studies12 ,15 ,16 and of both origins in two studies.13 ,14 Mean baseline LVEF of the participants varied from 24% to 37%. The dose of fish oil (calculated as the total dose of EPA and DHA) ranged from 600 to 4300 mg/day, with the ratio of EPA to DHA varying from 0.60 to 1.53. Duration of the investigation varied from 3 to 12 months. None of these studies reported adverse events related to fish oil supplementation.
Overview and characteristics of the included studies
Data quality
The quality score of the seven studies ranged from 3 to 5. All studies were randomised and placebo controlled, with six studies conducted in a double blind fashion10–12 14–16 and one in a single blind fashion.13 Three studies reported methods of random sequence generation,13–15 and three reported allocation concealment.10 ,14 ,15 Details of withdrawals were reported in six of the included studies.10–13 ,15 ,16
Effects of fish oil supplementation on cardiac function and remodelling
Left ventricular ejection fraction
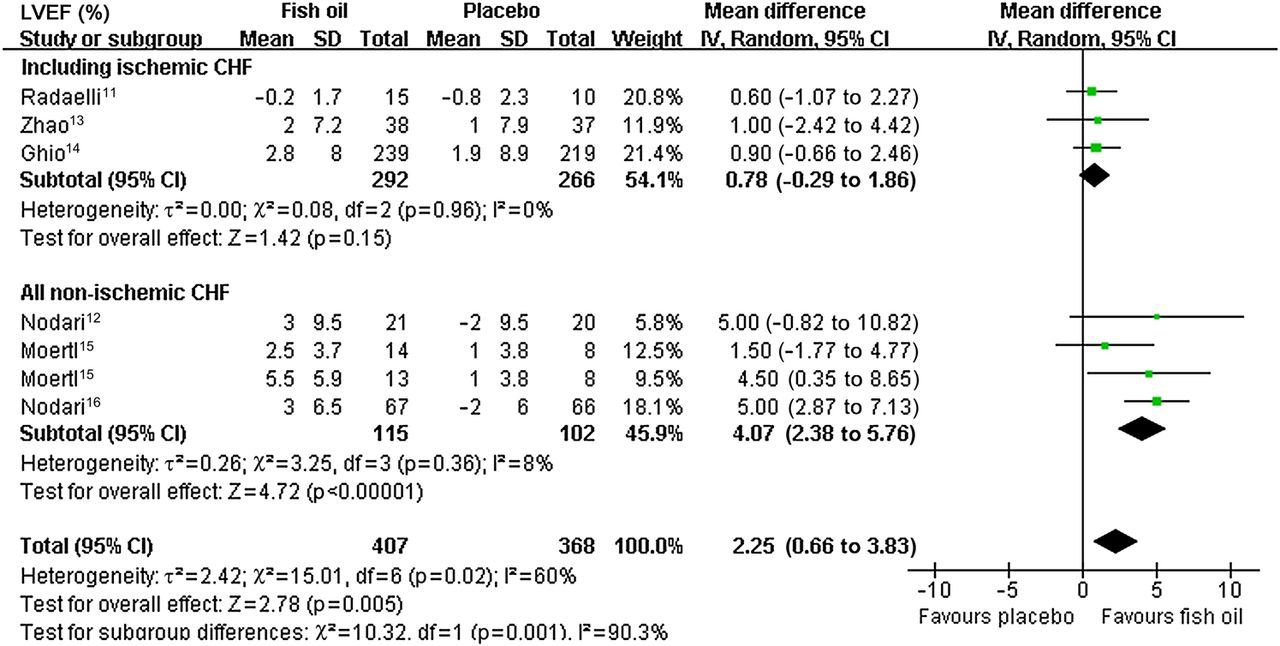
Six studies11–16 with seven study arms investigated the effects of fish oil on LVEF in CHF patients. Significant heterogeneity was detected among the seven study arms (I2=60%, p=0.02) and therefore the random effect model was applied. The pooled results indicated additional supplementation with fish oil significantly increased LVEF (seven study arms, 775 patients; WMD=2.25%, 95% CI 0.66 to 3.83, p=0.005) (figure 2), suggesting a beneficial effect of fish oil on cardiac systolic function.

Forest plot from meta-analysis of weighed mean difference in left ventricular ejection fraction (LVEF) for patients with chronic heart failure (CHF), randomised to fish oil or placebo.
In view of the fact that significant heterogeneity existed across the enrolled study arms, we performed predefined meta-regression analysis to explore the potential source of heterogeneity. The results indicated that the aetiology of CHF may be a potential modifier of the effect of fish oil on LVEF, and the percentage of patients with ischaemic CHF was negatively related to effect size (regression coefficient=−0.037, 95% CI −0.073 to −0.001, p=0.046), which largely explained the heterogeneity (figure 2). Other covariates, including mean age, gender of the participants, baseline LVEF, total dose of fish oil, ratio of EPA to DHA and follow-up duration were not significant modifiers.
Subsequently, we performed a subgroup analysis to specify the influence of CHF aetiology on the effects of fish oil on LVEF. We grouped the seven study arms according to the median percentage of patients with ischaemic CHF (0%). Therefore, subgroup analyses were performed in study arms which partially or wholly included patients with ischaemic CHF, and in study arms which included non-ischaemic CHF patients exclusively. For studies which partially or wholly included patients with ischaemic CHF,11 ,13 ,14 fish oil supplementation did not significantly affect LVEF (three study arms, 558 patients; WMD=0.78%, 95% CI −0.29 to 1.86, p=0.15) (figure 2), and no significant heterogeneity among these studies was detected (I2=0, p=0.96); however, for studies including non-ischaemic CHF patients exclusively,12 ,15 ,16 fish oil supplementation increased LVEF significantly (four study arms, 217 patients; WMD=4.07%, 95% CI 2.38 to 5.76, p<0.00001) (figure 2), and no significant heterogeneity among these studies was found either (I2=8%, p=0.36).
Left ventricular end-systolic volume and left ventricular end-diastolic volume
Four studies10 ,12 ,14 ,16 reported the effects of fish oil supplementation on LVESV, among which no significant heterogeneity was found (I2=0, p=0.84). The pooled results estimated with the fixed effect model indicated that fish oil reduced LVESV (four studies, 673 patients; WMD=−7.85 ml, 95% CI −15.57 to −0.12, p=0.05) (figure 3A). Only three studies10 ,14 ,16 reported the effects of fish oil on LVEDV, and no significant heterogeneity was detected (I2=0, p=0.92). The results indicated a decrease in LVEDV after fish oil supplementation although this was not statistically significant (three studies, 632 patients; WMD=−4.44 ml, 95% CI −14.52 to 5.65, p=0.39) (figure 3B).
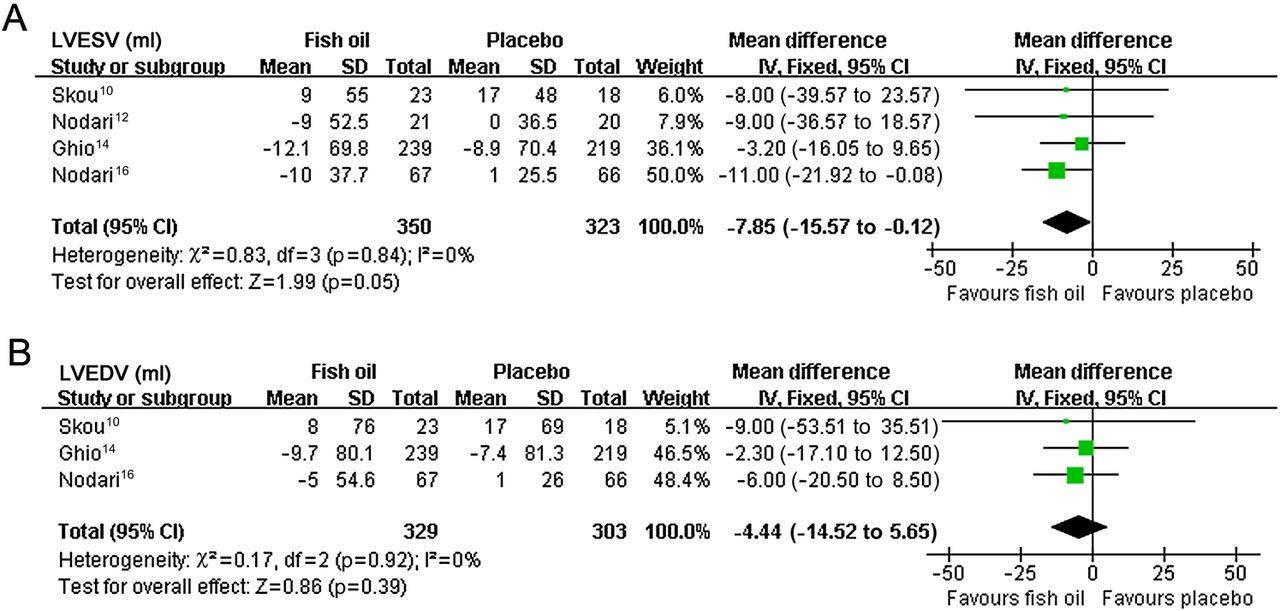
Forest plots from meta-analysis of left ventricular end-systolic volume (LVESV) (A) and left ventricular end-diastolic volume (LVEDV) (B) for patients with chronic heart failure, randomised to fish oil or placebo.
Effects of fish oil supplementation on functional capacity
NYHA functional class
For the three10 ,11 ,16 studies containing data on NYHA functional class, fish oil failed to result in a significant improvement in NYHA classification (three studies, 208 patients; WMD=−0.21, 95% CI −0.68 to 0.23, p=0.32) (figure 4A). Significant heterogeneity was detected (I2=90%, p<0.0001). Of these studies, one study16 included exclusively non-ischaemic CHF patients and fish oil significantly improved NYHA classification in these patients (133 patients; mean difference=−0.58, 95% CI −0.75 to −0.41, p<0.00001). The other two studies10 ,11 included exclusively ischaemic CHF patients, and fish oil supplementation had no significant effect in NYHA classification in these patients (two studies, 75 patients; WMD=0.01, 95% CI −0.20 to 0.21, p=0.93) without any significant heterogeneity (I2=0, p=0.34).

Forest plots from meta-analysis of New York Heart Association (NYHA) classification (A) and peak oxygen consumption (peak VO2) (B) for patients with chronic heart failure, randomised to fish oil or placebo.
Peak oxygen consumption
Three studies12 ,15 ,16 with four study arms, which included non-ischaemic CHF patients exclusively, investigated the effects of fish oil on peak VO2 in the exercise test. No significant heterogeneity was detected (I2=0, p=0.67) and the pooled results indicated fish oil significantly increased peak VO2 in non-ischaemic CHF patients (four study arms, 199 patients; WMD=1.68 ml/kg min, 95% CI 0.52 to 2.84, p=0.005) (figure 4B).
Publication bias
Publication bias was tested based on the data for fish oil supplementation on LVEF, which included the most study arms. Funnel plot (figure 5) and results of the Egger regression test suggested no significant publication bias (Egger test, p=0.302).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot (with pseudo 95% CIs) of all individual study arms in the meta-analysis left ventricular ejection fraction for patients with chronic heart failure, randomised to fish oil or placebo. WMD, weighed mean difference.
Discussion
In this study, we performed a meta-analysis of seven published clinical trials to investigate the effects of fish oil supplementation on cardiac function, remodelling and functional capacity in CHF. The results indicated additional fish oil supplementation caused a significant increase in LVEF and a reduction in LVESV in CHF, and the improvement in LVEF seemed to be more remarkable in patients with non-ischaemic CHF. Moreover, the benefits of fish oil were further demonstrated by improvement in NYHA classification and increase in peak VO2, although these results were obtained from limited studies in patients with non-ischaemic CHF. These results indicated that improvement in cardiac systolic function, ventricular remodelling and functional capacity may be important mechanisms underlying the potential therapeutic role of fish oil for patients with CHF, especially those with non-ischaemic CHF.
A large number of structural and functional abnormalities may be involved in the pathogenesis of CHF,1 and previous studies indicated that the benefits of fish oil supplementation in cardiac function and remodelling may be mediated by multiple effects on many of these processes and mechanisms.8 ,9 Fish oil could preserve cardiac mitochondrial function by stimulating expression of proteins involved in cardiac lipid metabolism,23 thereby reducing myocardial oxygen consumption and resulting in greater mechanic efficiency of the ventricle.24 Also, by inhibition of the inflammatory nuclear transcription factor, nuclear factor κB25 and stimulation of the anti-inflammatory hormone adiponectin,26 fish oil may exert its anti-inflammatory effect in CHF. This is considered to be an important therapeutic mechanism because persistent inflammation has been suggested to play a pathogenic role in CHF by impairment of myocardial contractility, inducing hypertrophy, promoting apoptosis and contributing to myocardial remodelling.27 Although other benefits have also been proposed, such as improvement in endothelial function, antioxidation, inhibition of neurohormonal activation, antihypertrophy and excitation–contraction coupling of the myocardium, the exact mechanisms underlying the therapeutic effects of fish oil in CHF have yet to be determined.8 ,9
Previous evidence from epidemiological studies demonstrated that fish consumption or fish oil intake was inversely associated with the incidence of CHF in the general population.28–30 Furthermore, the results of the GISSI-HF trial,31 the only published large scale study to date which has evaluated the effects of fish oil on clinical endpoints in patients with CHF, showed that long term treatment with fish oil reduced mortality and hospitalisations for cardiovascular reasons in patients with CHF on evidence based therapy, which strongly indicated a therapeutic role for fish oil in CHF. However, reduction in fatal arrhythmias and SCD can only contribute up to 50% of the total benefit of fish oil on mortality, suggesting other mechanisms may be involved.32 Results of our meta-analysis suggested that improvement in cardiac systolic function and ventricular remodelling may be important mechanisms underlying the beneficial effects of fish oil for CHF, despite its anti-SCD effects. Accumulating evidence suggested that LVEF, LVESV and LVEDV are strong predictors of mortality risk for patients with CHF,33–35 and a recent meta-analysis also indicated that therapeutic strategies which improve cardiac function and remodelling may confer benefits on mortality in these patients.36 In fact, according to the results of a previous study including a large contemporary CHF population, our finding of 2.25% improvement with additional fish oil supplementation would correspond to about a 6% lower risk of overall mortality.37 Although the effect of fish oil on LVEF and mortality risk in CHF seemed to be modest, it could be important clinically in a larger population. More importantly, our results were obtained based on randomised, blinded, placebo controlled trials in patients who had already taken the current optimal medications for CHF, indicating a further beneficial effect of fish oil supplementation for CHF on the basis of treatment strategies recommended by the current guidelines.
Interestingly, the results of meta-regression and subgroup analysis indicated that the benefit of fish oil on cardiac function seemed more remarkable in patients with non-ischaemic CHF compared with those with ischaemic CHF. The exact mechanisms underlying this difference are not clear. However, a recent review suggested that significant heterogeneity exists in trials of fish oil in patients with cardiovascular disorders, and some benefits of fish oil depended on the population studied.38 For patients with non-ischaemic CHF, our study found that fish oil supplementation significantly improved LVEF by 4.07%. Although a quantitative association between LVEF and risk of mortality in patients with non-ischaemic CHF has not been reported in previous studies, it has been suggested that increased LVEF was related to a lower risk of total mortality in these patients.39
Results of our meta-analysis also indicated that additional supplementation of fish oil can lead to improvement in NYHA classification and an increase in peak VO2 although these results were obtained on the basis of studies in non-ischaemic CHF and mainly driven by one study.16 Moreover, peak VO2 has also been suggested to be of important prognostic value for mortality in patients with CHF, suggesting that the beneficial effects of fish oil on total mortality in CHF may be related to improvement in the functional capacity of patients.40 ,41
Several potential limitations should be addressed regarding the present meta-analysis. First, the number of studies and patients included in this meta-analysis was small, so the results of some of the estimations, such as the effects of fish oil supplementation on NYHA classification and LVEDV, should be interpreted with caution. Second, as for the meta-regression and subgroup analysis, the number of included studies and patients in each stratum was relatively small. Also, we did not have access to individual patient data. The results of the subgroup analysis might be different if larger numbers of studies were included or individual patient data were available (eg, the subgroup could be defined as patients with ischaemic CHF and non-ischaemic CHF, and not as studies partially or wholly including patients with ischaemic CHF and studies including patients with non-ischaemic CHF exclusively in the current analysis).
In conclusion, our meta-analysis suggested that improvements in cardiac function, remodelling and functional capacity may be important mechanisms underlying the benefit of fish oil on mortality in patients with CHF who are already on current optimal medications for CHF, particularly in those with non-ischaemic CHF. Additionally, large scale randomised controlled trials are needed to uncover all of the potential benefits of fish oil supplementation in patients with CHF of different aetiologies.
Acknowledgments
The authors would like to thank Dr Deddo Moertl et al for sharing the unpublished baseline data of their study for this analysis.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; not externally peer reviewed.