Article Text

Abstract
OBJECTIVE To describe clinical outcomes of a paediatric population with histologically confirmed lymphocytic myocarditis.
DESIGN A retrospective review between November 1984 and February 1998.
SETTING A major paediatric tertiary care hospital.
PATIENTS 36 patients with histologically confirmed lymphocytic myocarditis.
MAIN OUTCOME MEASURES Survival, cardiac transplantation, recovery of ventricular function, and persistence of dysrhythmias.
RESULTS Freedom from death or cardiac transplantation was 86% at one month and 79% after two years. Five deaths occurred within 72 hours of admission, and one late death at 1.9 years. Extracorporeal membrane oxygenation support was used in four patients, and three patients underwent heart replacement. 34 patients were treated with intravenous corticosteroids. In the survivor/non-cardiac transplantation group (n = 29), the median follow up was 19 months (range 1.2–131.6 months), and the median period for recovery of a left ventricular ejection fraction to > 55% was 2.8 months (range 0–28 months). The mean (SD) final left ventricular ejection and shortening fractions were 66 (9)% and 34 (8)%, respectively. Two patients had residual ventricular dysfunction. No patient required antiarrhythmic treatment. All survivors reported no cardiac symptoms or restrictions in physical activity.
CONCLUSIONS Our experience documents good outcomes in paediatric patients presenting with acute heart failure secondary to acute lymphocytic myocarditis treated with immunosuppression. Excellent survival and recovery of ventricular function, with the absence of significant arrhythmias, continued cardiac medications, or restrictions in physical activity were the normal outcomes.
- myocarditis
- paediatric cardiology
- immunosuppression
Statistics from Altmetric.com
The diagnosis of acute myocarditis in childhood presents a formidable clinical challenge, as the spectrum of presentation can manifest from little or no detectable myocardial dysfunction to fulminant congestive heart failure.1-3 Limitations in defining the nature of the disease—its incidence, clinical course, and response to treatment—have been in part caused by the lack of a uniform standard in the diagnosis. As such, existing literature addressing clinical outcomes have relied upon various diagnostic criteria, and report a broad range in survival and residual cardiac dysfunction.4-8 In this regard, there is limited literature derived from a homogenous paediatric population, with histologically confirmed acute lymphocytic myocarditis.9-13 Using the Dallas classification proposed in 198414 as a diagnostic platform, we describe the clinical outcomes from a paediatric population with biopsy confirmed myocarditis, following immunosuppressive treatment.10-12
Methods
STUDY POPULATION
The study population comprised children presenting to the Hospital for Sick Children, Toronto, a tertiary paediatric referral centre, between November 1984 and February 1998 with acute heart failure, an unexplained dysrhythmia, or both, in the setting of an anatomically normal heart, who had undergone a diagnostic endomyocardial biopsy which demonstrated lymphocytic myocarditis. During this period, 273 such biopsy procedures were performed.
ENDOMYOCARDIAL BIOPSIES
Biopsies were performed with right heart haemodynamics and cardiac output determinations (thermodilution or Fick method) from standard percutaneous femoral or internal jugular venous approaches using a 6F bioptome (Mansfield Scientific, Boston, Massachusetts, USA). General anaesthesia was employed in the majority of procedures. A small number of patients who required the institution of extracorporeal membrane oxygenation (ECMO) support immediately after admission had biopsies taken from the atrium during cannulation. Some patients underwent one or two subsequent biopsies as part of an algorithm regarding continuation of immunosuppressive treatment. In the pathology laboratory, biopsies for light microscopic assessment were placed in one cassette, rapidly processed (four hours), and embedded in one paraffin block. Histological sections 4 μm in thickness were cut through the block using a rotary microtome to produce a continuous “ribbon” of tissue sections which were mounted onto glass slides and coverslipped. Typically, 25–30 glass slides were thus produced to sample all levels throughout a set of biopsies. Odd numbered slides were stained with haematoxylin and eosin and even numbered slides were left untouched for special stains if subsequently needed. Biopsy specimens were reviewed by two paediatric cardiovascular pathologists and classified according to the Dallas criteria.14
DATA COLLECTION
The health record and cardiology database for each patient were reviewed to obtain information regarding presentation, in-hospital course and management, outpatient follow up, ECGs, Holter examinations, echocardiographic studies, and cardiac catheterisation haemodynamic data. Additional clinical follow up data on four patients no longer followed at our institution were obtained through telephone contact with the patients’ cardiologists.
MANAGEMENT AND TREATMENT
All patients presenting with acute congestive heart failure (in the absence of structural heart disease) and a working diagnosis of possible myocarditis or cardiomyopathy were admitted either to the inpatient cardiology ward or intensive care unit. Since 1995, all patients were admitted directly to the intensive care unit in order to provide expeditious support in the form of mechanical ventilation, inotropic agents, transvenous ventricular pacing, antiarrhythmic treatment, or mechanical heart assist devices. Once they were haemodynamically stable, patients underwent a diagnostic right heart catheterisation and endomyocardial biopsy. If lymphocytic myocarditis was present on the biopsy, immunosuppressive treatment was begun with corticosteroids (intravenous methylprednisolone 10 mg/kg/day over two hours for three days followed by a tapering intravenous or oral dosage regimen to 0.3 mg/kg/day by day 7 or 8, continued for two to three months). The additional administration of gammaglobulin (one dose of 2 g/kg) in this setting was started after reports that it was an adjunctive immunosuppressive agent.10 Once the patient was haemodynamically stable, management continued on the inpatient cardiology ward until the time of discharge. The indication for ECMO was a sudden or progressive reduction in cardiac output despite maximal inotropic and ventilatory support. The goal of such support was initially as a bridge to heart transplantation but, based upon an institutional experience of recovery of cardiac function, a period of observation has been allowed before a decision for transplantation is made.15 ,16
CARDIAC FUNCTION
Cardiac function was evaluated echocardiographically. Parameters assessed included ejection and shortening fractions, corroborated by a qualitative assessment of ventricular function which included the presence or absence of wall motion abnormalities, evidence of significant valvular regurgitation, evaluation of diastolic ventricular function,17 and the presence of a pericardial effusion. Measurements noted were left ventricular end systolic and diastolic dimensions, and the thickness of the left ventricular posterior wall. Historically, our echocardiographic laboratory relied upon M mode technology for ejection and shortening fraction determinations. In the presence of an abnormal interventricular septal curvature, ejection fraction was calculated by a single or biplane Simpson’s method. If unavailable, such measurements were calculated by single plane offline analysis18 on a computer assisted system (Hewlett Packard, Andover, Massachusetts, USA). Analyses were made of echocardiographic assessments at the time of presentation and at the most recent follow up. The time period to achieve a left ventricular ejection fraction of > 55% was noted. Indirect assessment of cardiac function was ascertained by the functional level of physical activity at the time of the most recent follow up as classified by the New York Heart Association (NYHA).19 Outpatient cardiac medications included corticosteroids, digoxin, angiotensin converting enzyme inhibitors, and diuretics. The time from hospital discharge to the discontinuation of medications was also noted.
DATA ANALYSIS
Data are presented as means (SDs), medians with ranges, and frequencies as appropriate. Where available, echocardiographic measurements were standardised for age (ejection and shortening fractions) or body surface area (left ventricular end systolic and diastolic dimensions, left ventricular posterior wall thickness) as a Z score from non-linear regression equations based on a normal population (S Colan, personal communication, 1996). The Z score was calculated as: patient value − population mean/population SD. Mean Z scores were tested against a null hypothesis of a population mean of 0 with a single sample t test. Freedom from death or cardiac transplantation was plotted using Kaplan-Meier estimates from time of hospital admission. Risk factors for cardiac transplantation or death were sought with Fisher’s exact test,t tests, and Kruskal-Wallis analysis of variance, as appropriate. Independent risk factors for cardiac transplantation or death were sought in stepwise multiple logistic regression analysis; p < 0.05 was set as the level of significance.
Results
Thirty six patients had biopsy proven myocarditis. One patient was excluded from analysis because of a lack of sufficient clinical data. Of the remaining 35 patients, 28 fulfilled Dallas criteria as positive and seven classified as borderline positive. The five patients who were too critically ill to undergo an endomyocardial biopsy and thus treated presumptively as myocarditis with later histological confirmation are included. A mean of 5 (2) biopsy specimens were obtained per patient. Specimens were obtained from the right ventricle in 27 patients and from the left ventricle in five patients. Atrial biopsy specimens were obtained from three patients during ECMO cannulation. One atrial biopsy had no evidence of active myocarditis but the explanted heart (at time of transplantation) showed classic changes of myocarditis. One patient with a borderline positive endomyocardial biopsy had florid myocarditis at necropsy. Eight patients had one subsequent endomyocardial biopsy procedure and three had a third biopsy procedure for the purpose of immunosuppression management. There was one biopsy complication, a ventricular perforation, which did not require surgical management.
INITIAL PRESENTATION AND IN-HOSPITAL COURSE
The median age at presentation was 3.3 years (range 1.0–15.1 years) with 13 boys and 22 girls. The median duration of symptoms before admission was seven days (range 1–47 days). A possible infectious aetiology was identified in eight cases; three siblings had positive parvovirus serology, two had influenza A from nasopharyngeal swabs, one had enterovirus and one adenovirus isolated by stool electron microscopy, and one had coxsackie B5 virus from serology.
The initial ECG was abnormal with evidence of ST segment flattening or T wave inversion in all patients, excluding those presenting with a ventricular rhythm. Low QRS voltages—that is, < 5 mm in any precordial lead—were present in 28 (80%) patients. Arrhythmias requiring treatment (atrioventricular block (n = 4), ventricular tachycardia (n = 5), or both (n = 1)) were present in 10 (29%) patients.
The initial ECG showed a mean left ventricular ejection fraction of 34 (14)% (n = 31) and shortening fraction 18 (8)% (n = 25). The mean Z scores were −4.28 (1.95) (p < 0.001 versus a normal population mean of 0) and −7.39 (3.54) (p < 0.001), respectively. There were four patients in which the ventricular function was so decreased that ejection fractions could not be measured. Significant valvular insufficiency consisted of moderate mitral regurgitation in 10 (29%) patients. No significant wall motion abnormalities were noted. Diastolic ventricular function was not assessed in the majority of initial studies. The mean Z scores were 3.87 (3.13) (p < 0.001, n = 16) for left ventricular end systolic dimension, 2.52 (2.59) (p < 0.001, n = 26) for left ventricular end diastolic dimension, and −0.41 (3.78) (p = 0.61, n = 23) for left ventricular posterior wall thickness. A pericardial effusion was present in 13 (37%) patients, none requiring intervention.
Twenty three (66%) patients were admitted to the intensive care unit; all required intravenous inotropic support, and 18 (51%) were mechanically ventilated. Four patients (12%) required transvenous ventricular pacing, and nine (26%) required antiarrhythmic treatment.
The median period from admission to endomyocardial biopsy was two days (range 0–17 days).
Thirty four patients received corticosteroid treatment within a median of two days (range 0–13 days) from admission and a median of 0 days (range −17–7 days) from biopsy. Intravenous gammaglobulins were administered to 15 (43%) patients within a median of one day (range 0–4 days) of biopsy. A second endomyocardial biopsy in four of eight patients showed ongoing inflammation requiring prolongation of oral corticosteroid treatment. All three third biopsies showed resolution of inflammation. Two patients also received azathioprine and one α interferon.
Four patients were placed on ECMO support, all within 48 hours of admission.
OUTCOMES
Figure 1 summarises the outcomes of the cohort with respect to survival, cardiac transplantation, and recovery of normal ventricular function. The outcomes of the patients who received ECMO support are also outlined. There were three (9%) deaths and two (6%) cardiac transplantations during the initial hospitalisation. Three patients were listed for cardiac transplantation on days 3, 3, and 12 after admission and two were recipients of donor hearts within two and 10 days of listing. The third patient, while listed for heart transplantation, recovered normal ventricular function and was separated from ECMO support after six days. One patient, weaned off ECMO after seven days, had persistently severe ventricular diastolic dysfunction, and died because of myocardial failure and fungal sepsis. In the six patients who had severe cardiorespiratory decompensation—that is, died or required ECMO support during the initial hospitalisation—such events all occurred within 72 hours of presentation. There was only one late death occurring 1.9 years after initial presentation. This patient demonstrated persistent ventricular dysfunction and significant ventricular arrhythmias. Resuscitated from a cardiac arrest, the patient underwent a heart transplantation, but died three days postoperatively from graft failure. Kaplan-Meier estimates of freedom from death or cardiac transplantation were 86% one month after admission (95% confidence intervals (CI) 74% to 97%) and remained at 79% (95% CI 63% to 96%) after two years (fig 2).

Flowchart of patient outcomes with biopsy positive myocarditis. ECMO, extracorporeal membrane oxygenation, LV, left ventricular.

Kaplan-Meier survival (freedom from death, cardiac transplantation, or both) estimates of patients with histologically proven myocarditis. Broken lines indicate 95% confidence intervals.
Clinical data and in-hospital course were reviewed to identify risk factors for death or heart transplantation (table 1). Univariate analysis identified older age at presentation, lower initial ejection fraction, need for mechanical ventilation or ECMO support, occurrence of a non-terminal cardiac arrest, and ventricular arrhythmias to be significant risk factors. Multivariate analysis indicated ventricular arrhythmias as the only significant independent predictor.
Comparision of initial characteristics and clinical course
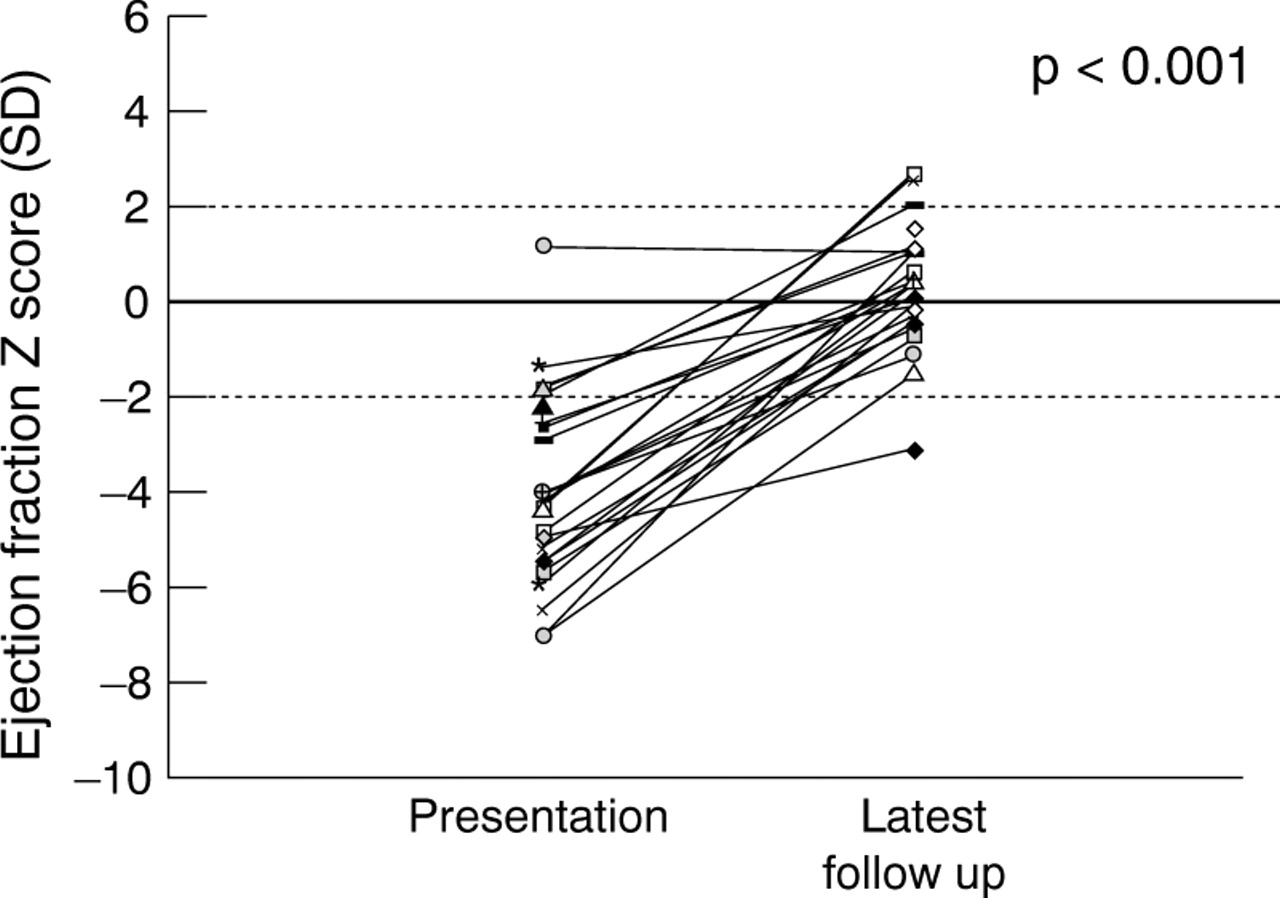
Table 2 outlines the clinical course in survivor/non-cardiac transplantation cohort (n = 29). There was a significant improvement in ejection and shortening fractions, with the majority of patients recovering normal ventricular function (fig 3) (table 2). There was no significant change in the left ventricular posterior wall thickness. The median period for recovery of left ventricular ejection fraction of > 55% was 2.8 months (range 0–28 months). Overall, left ventricular end systolic and diastolic dimensions, at the most recent follow up, were within the normal range (fig 4) (table 2). No patient had more than mild valvular regurgitation at the time of the most recent echocardiographic study or evidence of diastolic dysfunction. Two patients had evidence of residual left ventricular dysfunction at the time of latest follow up. In one patient, asymptomatic six years after presentation and on no cardiac medication, the ejection and shortening fractions were 50% and 22%, respectively, with qualitative evidence of decreased ventricular function. Exercise testing four years after presentation showed mild to moderate exercise intolerance with a maximum oxygen consumption 67% of predicted. The follow up echocardiogram from the second patient at 3.8 months after presentation (most recent follow up) showed significant improvement with left ventricular ejection and shortening fractions of 42% and 20%, respectively.
Course of survivor/non-cardiac transplantation cohort

Plot of left ventricular ejection fractions (n = 26). The Z score is adjusted for age at initial presentation and latest follow up of patients who survived (early and late) without cardiac transplantation. Median period of follow up was 19 months (range 1.2–131.6 months). All data plotted with connecting lines for patients from whom both initial and most recent data were available.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Plot of left ventricular end diastolic dimensions (n = 20). The Z score is adjusted for body surface area at initial presentation and latest follow up of patients who survived (early and late) without cardiac transplantation. Median period of follow up was 19 months (range 1.2–13.6 months). All available data plotted with connecting lines for patients from whom both initial and most recent data were available.
In the five patients who presented in third degree heart block, the initial ejection fractions were 11%, 25%, 34%, 44%, and 52%. Four patients required transvenous ventricular pacing for one, four, and nine days and one patient required a permanent pacemaker implantation. All patients had sinus rhythm restored and four patients had completely normal ECGs on follow up. One patient continues with residual cardiac dysfunction (see above) with evidence of complete left bundle branch block on the resting ECG and periods of 2:1 atrioventricular block on exercise testing. Holter examinations on two patients both at three months’ follow up showed periods of first degree atrioventricular block in one and T wave alternans in the other. One additional patient has persistent ST segment abnormalities, associated with decreased but improving ventricular function (follow up 3.8 months). The one survivor with ventricular tachycardia on presentation had no evidence of any arrhythmia 27 months later.
Two patients, those with the shortest follow up (1.2 and 3.8 months), remain on cardiac medications. At the most recent assessment, all parents and patients reported no cardiac symptoms or restriction in physical activities, and were classified as NYHA functional class I.
Discussion
Studies report better outcomes in patients with myocarditis compared with those with idiopathic cardiomyopathy.7 ,9 ,11 ,12 ,20-23 The extrapolation of outcomes in the adult to the paediatric population cannot be assumed. A consistently reliable modality for the diagnosis of myocarditis remains elusive. Clinical presentation,2 ,7 ,9 ,11 ,20 ECG changes, echocardiographic features, laboratory investigations including virologic testing,24 radionuclide studies,25 and endomyocardial biopsy have limitations. As a result, conclusions regarding outcomes in this heterogeneous group presenting in acute heart failure or arrhythmia have limitations. To our knowledge, this is the largest review reporting clinical outcomes in a selected subgroup of patients with myocarditis—that is, children with histologically confirmed acute myocarditis.
The true incidence of myocarditis is not known. Forensic studies have demonstrated incidences of 9%1 and 17%26 in sudden paediatric deaths. Noren et alreported necropsy confirmation of myocarditis in 4.2% of violent deaths in a paediatric population, suggesting that the prevalence of “silent” clinically asymptomatic myocarditis may be higher than is generally suspected.1 The incidence of histologically proven myocarditis among patients of all ages presenting with acute heart failure, or a “dilated cardiomyopathy”, varies from 4–67% depending on diagnostic criteria, patient selection, and timing of biopsy.2-4 ,7 ,9 ,11 ,24
ENDOMYOCARDIAL BIOPSY
The use of endomyocardial biopsy in patients presenting with acute heart failure is increasing.27 Despite challenges to its accuracy,28 the application of the Dallas criteria has improved interobserver variability, from 95% concordance after the first review, to 100% concordance after a second review,29 although significant false negative rates have been reported, ranging from 2–58%.30 ,31 As a result, studies based on positive endomyocardial biopsy alone may exclude a number of patients with acute myocarditis. Spontaneous recovery of ventricular function in patients with so called idiopathic cardiomyopathy has been reported4 ,7 ,9 ,11 and it remains unclear whether these patients truly represented a reversible “unknown” myopathic process or a proportion having biopsy negative acute myocarditis. In this report, we excluded those patients who, despite a clinical presentation consistent with acute myocarditis, had a negative biopsy or no biopsy.
In the myocarditis multicentre trial, Mason and colleagues reported positive biopsies for myocarditis in 214 of 2233 (10%) patients presenting with clinically suspected myocarditis.7 ,8Similarly, the incidence of positive biopsies using the Dallas criteria were 7% by Grogan and colleagues6 and 4.4% by Chow and colleagues3 in adults presenting with acute heart failure or a dilated cardiomyopathy. In the paediatric population, our study showed that 13% of 273 biopsies were positive for myocarditis, while Matitiau and colleagues9 and Kleinert and colleagues11 reported that 40% and 38% of biopsies, respectively, were positive by the Dallas criteria.
SURVIVAL
Survival of adult patients with idiopathic dilated cardiomyopathy is 23–40% at five years,21 ,22 and survival for myocarditis, based on the Dallas criteria, has been reported between 44–83%.4 ,6 ,7 In the paediatric population, survival of dilated cardiomyopathy ranges from 60–70% at one year, and from 34–56% at five years.20 ,23 In many of these studies, histologic evaluation of cardiac tissue during the acute illness was not available, and management did not include immunosuppressive treatment. Matitiau and colleagues reported a mortality of 30% in 24 children < 2 years of age with dilated congestive cardiomyopathy.9 Within this group, nine patients had histologic evidence of myocarditis by the Dallas criteria with a survival rate of 78% at one to five years, in contrast to 40% in those without myocarditis. The survival rate was 100% in paediatric studies by Gagliardi and colleagues12 and more recently by Kleinert and colleagues,11 with follow up periods of one year and 17 months, respectively; in our study the survival rate was 79%. The outcomes of our study and those of Matitiau and colleagues,9 Kleinert and colleagues,11 and Gagliardi and colleagues12 document improved survival in the paediatric population. Furthermore, younger age within this population is associated with improved survival.9
If death occurred, it was almost always within the first few days after presentation. In our study, survival beyond 72 hours without the need for ECMO support increased the likelihood for overall survival to 97%. This finding is consistent with that of Matitiau and colleagues,9 who noted that all four deaths in their series occurred within hours of presentation to hospital.
One late death (1.9 years) was a patient referred to our centre 34 days after presentation. This patient demonstrated persistent ventricular dysfunction and significant ventricular arrhythmia requiring antiarrhythmic treatment. Corticosteroids were administered, late from initial presentation, perhaps beyond a time when a critical mass of myocyte mass was damaged.
CARDIAC FUNCTION
There is compelling evidence to suggest that myocarditis can evolve into a chronic disease, which can progress to a form of dilated cardiomyopathy.9 Adult studies have reported persistent or progressive ventricular dysfunction in > 70% of biopsy positive patients.4 In a paediatric population, Matitiau and colleagues9 reported an ejection fraction < 50% in 29% of patients followed from 1–7.5 years, and Gagliardi and colleagues12 reported a mean ejection fraction of 55% after one year follow up in 20 patients, with 50% of those patients having an ejection fraction of < 55%. Notably, an impressive 100% recovery of ventricular function was found by Kleinert and colleagues in nine patients who received immunosuppressive treatment.11
In our study, 93% of the survivors had a final ejection fraction > 55% and qualitatively normal ventricular function. Although all survivors were reportedly active, asymptomatic in NYHA functional class I, provocative evaluation of ventricular function with exercise testing was not performed.
ARRYTHMIAS
The incidence of arrhythmias on initial presentation was 29% in this series. Friedman and colleagues reported that 12 (26%) patients, mean age 12 years, presenting with ventricular arrhythmias had positive biopsies (Dallas criteria).13 Similarly Wiles and colleagues documented myocarditis in 9% of children presenting with complex ventricular arrhythmias.32
Friedman and colleagues reported significant residual ventricular arrhythmias requiring medication in 42% of their patients at a mean follow up period of 51 months, and histologic resolution did not correlate with resolution of arrhythmias.13 In contrast, Vignola and colleagues reported 100% resolution in six biopsy positive adults with normal electrophysiologic testing, and subsequent negative biopsies for inflammation.33 In our study, only one patient required prolonged antiarrhythmic treatment for a persistent ventricular arrhythmia, associated with poor ventricular function; this patient subsequently died.
IMMUNOSUPPRESSIVE TREATMENT
The use of immunosuppressive or antiviral treatment (corticosteroids, immunoglobulins, cyclosporine, azathioprine, or α interferon) remains controversial in the treatment of acute myocarditis.7 ,9-12 34-36 During the early viral replication phase, some patients fail to contain the virus and fulminant massive myocardial cell necrosis occurs. In this phase, the potentially beneficial effects of such treatment have been brought into question with animal studies demonstrating detrimental sequelae by enhancement of myocardial damage.37 ,38 There is increasing evidence, however, from both animal and human trials to suggest that immunosuppressive treatment can have a positive impact on the host defence response in myocarditis.10-12 ,33 ,36 ,39
The myocarditis treatment trial, a prospective, randomised controlled trial in adults analysing possible benefits of immunosuppressive treatment, showed no significant improvement in mortality or ventricular function.7 ,8 However, this study included patients with symptom durations as long as two years, bringing into question the extrapolation of its results to a paediatric population with shorter symptom durations.5 ,39 ,40 Most adult studies report longer symptom durations, possibly reflecting patient tolerance or reluctance to seek medical attention.3 ,4 ,34 ,35 As such, persistent or chronic myocarditis may represent a unique subset which has a less favourable response to immunosuppressive treatment.
Our patient population, with the exception of one patient, universally received a course of corticosteroids within a mean of three days from admission to hospital. Treatment with other immunomodulators, including azathioprine and α interferon, was not widely administered. Our data further support the notion that improved survival in a paediatric population may be a result of the use of corticosteroids as immunomodulator treatment during an “optimal window” in disease evolution.9 ,11 ,12
ECMO AND CARDIAC TRANSPLANTATION
A few patients develop aggressive irreversible myocyte injury from the initial impact of the viral infection. In this group, medical treatment does not appear to alter the unrelenting fulminant course. ECMO support alone, or as a bridge to cardiac transplantation, may be the only life saving therapeutic modality at this end of the clinical spectrum. Individual reports15 ,16 and our own experience describe a total of eight patients who were supported on ECMO. Five of these patients were successfully separated, of which three had restoration of normal cardiac function, one had residual myocardial dysfunction, and one died of fungal sepsis. One patient died while on support, and two additional patients (in our series), underwent cardiac transplantation. With ECMO and heart transplantation as part of the treatment armamentarium, our overall institutional survival was 89%.
STUDY LIMITATIONS
Lack of an unequivocal diagnostic tool for myocarditis directed our selection criteria—that is, the subgroup of patients with myocarditis with histological confirmation by Dallas criteria. Advances in immunohistochemistry may redefine histologic criteria for the diagnosis; however, at present the Dallas criteria remains the most standardised and reliable mode of diagnosis and patient selection. As such, we cannot comment on the outcomes of those patients with myocarditis who were biopsy negative or not biopsied. Over the study period, the treatment strategy for myocarditis was in evolution. This is reflected in some of the lack of uniformity in our monitoring and management of these patients, particularly with respect to non-corticosteroid immunomodulative treatment. Our institutional management of acute myocarditis has consisted of a high rate of initial intensive care monitoring, mechanical ventilation, and intravenous inotropic support. Corticosteroid treatment was almost universally used in our patient population. In the absence of prospective randomised clinical trials, it is not yet determined what the individual contributions of these factors are in our successful outcomes. In particular, this experience further underscores the need for such trials comparing the natural history of patients with acute myocarditis not treated versus those treated with immunosuppressive therapy in this paediatric population.
CONCLUSION
Our experience demonstrates excellent outcomes in patients with acute heart failure with biopsy confirmed myocarditis, particularly those surviving the first 72 hours after presentation. High rates of survival, recovery of ventricular function, and absence of significant arrhythmias, continued cardiac medications, and restrictions of physical activity were found.